Functional outcome of arthroscopic Eden–Hybinette procedure with iliac-crest bone graft in recurrent anterior shoulder instability
Thomas Mathew Theckedath, John Thayyil John, Joice Varghese M J, Renjit J Mathew, Shinas B Salam, David Joseph
Abstract
Introduction: Glenoid bone defects play a significant role in anterior shoulder instability. Critical anterior glenoid bone loss is a recognized cause of failure after soft-tissue stabilization and often requires bone-augmentation procedures. Arthroscopically modified Eden-Hybinette procedures using iliac crest bone graft are gaining popularity as effective options in recurrent anterior shoulder instability with critical glenoid bone loss especially after failed Bankart repair or Latarjet procedure. This paper reports the mid-term clinical and functional outcomes of arthroscopic Eden-Hybinette procedure with iliac crest autograft in patients with recurrent anterior shoulder instability.
Materials and methods: Retrospective analysis of a case series of 18 patients with recurrent anterior shoulder instability and critical glenoid bone loss who underwent arthroscopic Eden–Hybinette procedure with iliac crest autograft between January 2018 and February 2025 was done. Glenoid and humeral bone defects were quantified using pre-operative CT scans. Data on patient demographics, pre-operative and post-operative clinical assessments, radiographic findings, and complications were analysed. Clinical assessment was done using the WOSI (Western Ontario Shoulder Instability) index and the Rowe scores pre-operatively and post-operatively at 3 months, 6 months, 12 months and 2 years.
Results: The mean age was 33.5 years. The mean number of preoperative dislocations was 4.1. The mean interval from first dislocation to surgery was 4.6 years. The mean operative time was 80 minutes and the mean duration of hospital stay was 2.5 days. The mean follow-up period was 38 months (ranging from 6 months to 7 years). The mid-term results indicate significant improvement in shoulder stability and function post-operatively. The mean post-operative Rowe score improved to 78.75 ± 12.24 (P-value<0.05) and the mean post-operative WOSI score improved to 23.86 ± 4.48 (P-value<0.05). No post-operative re-dislocation episodes were noted till the last follow up. One patient had a single subluxation episode at 2 years of follow up which settled with physiotherapy and did not recur. Fourteen patients (77.78%) regained normal range of motion (ROM). The four patients with remplissage had less than 25° loss of external rotation. Complications included two superficial wound infections and donor-site sensory disturbances.
Conclusion: The arthroscopic Eden-Hybinette procedure with iliac crest bone graft is an effective option for recurrent anterior shoulder instability with significant bone loss, yielding favourable functional outcomes and improved quality of life of patients. In this series with mid-term follow-up, arthroscopic Eden–Hybinette procedure with iliac-crest autograft yielded significant improvement in shoulder stability and function with low recurrence and acceptable complication rates. It is a viable alternative to the Latarjet procedure in selected patients with critical glenoid bone loss, preserving options for revision with Latarjet if needed. Larger comparative and longer-term studies are recommended.
Introduction
Recurrent anterior shoulder instability with critical glenoid bone loss is increasingly recognized as a factor predicting failure after arthroscopic Bankart repair. Bone-augmentation procedures like Latarjet, Eden–Hybinette (free bone block) and distal tibial allograft aim to restore glenoid articular surface and stability. The Eden–Hybinette procedure, historically an open bone block technique, has evolved to an all-arthroscopic approach with modern fixation options using cerclage tape or screws, and uses iliac-crest cancellous autograft which may favour graft incorporation. This manuscript presents outcomes from 18 patients treated with arthroscopic Eden–Hybinette procedure for glenoid bone loss of 20% or more at a single centre.
Many bone augmentation procedures have been developed to treat recurrent anterior shoulder instability. The success of these procedures depends on several factors such as the patient’s age, level of athletic participation, involvement in contact sports before and after surgery, presence of joint hyperlaxity, and the degree of bone loss in the glenoid or humeral head. These parameters play a critical role in determining outcomes after soft-tissue arthroscopic Bankart repair [1,2]. Recurrent shoulder dislocations may lead to a spectrum of injuries, from a soft-tissue Bankart lesion of the anterior glenoid labrum to variable glenoid bone loss, sometimes associated with a Hill-Sachs defect. Accurate identification of these risk factors through CT and MRI imaging is crucial for evaluating the extent of glenoid bone loss, measuring Hill-Sachs lesion depth, and determining whether the lesion is “off-track,” all of which guide appropriate treatment planning.
Surgical procedures aimed at restoring glenoid bone structure include the Eden-Hybinette, Latarjet, J-bone graft, and distal tibial allograft techniques. The Latarjet procedure is most frequently used as a revision operation following a failed Bankart repair but can also be selected as a primary procedure in patients with a high instability severity index score. Glenoid bone loss is generally considered significant when more than 20% of the inferior glenoid is affected [3] or when the defect’s supero-inferior dimension exceeds half the glenoid’s maximum antero-posterior diameter. Radiographic findings such as disappearance of the sclerotic glenoid line on AP radiographs, as described by Jankauskas et al, can indicate anterior glenoid bone loss [4]. These findings typically warrant further cross-sectional imaging to evaluate the extent of critical bone loss.
Long-term results of the Latarjet procedure show a recurrence rate of approximately 5–6%, motivating surgeons to adopt more comprehensive reconstructive options to reduce the likelihood of failure [5]. The Eden-Hybinette procedure has proven particularly effective in cases of failed Latarjet procedures or when the glenoid bone defect is too large for a coracoid graft. It is also useful when the coracoid process is abnormally shaped or when glenoid fractures are not repairable. The success of this procedure lies in its ability to restore the glenoid’s bony anatomy by matching the inner surface of the iliac crest bone graft precisely to the glenoid defect. Initially introduced as a bone grafting procedure combined with capsulorrhaphy, it has evolved significantly since its inception in 1917 into an all-arthroscopic technique with modern fixation options like cerclage tape or screws. This modern approach preserves the coracoid process and minimizes damage to the subscapularis muscle, offering clear advantages over other bone block methods.
Materials and methods
The data on eighteen patients satisfying the inclusion and exclusion criteria who were diagnosed with recurrent anterior shoulder instability with critical bone loss and treated surgically with arthroscopic bone block procedure with iliac crest autograft at a single centre between January 2018 and February 2025 was retrospectively analysed. Patients with recurrent anterior shoulder instability and glenoid bone loss of 20% or more underwent the arthroscopic bone block procedure. In patients with an engaging/off-track Hill–Sachs lesion, remplissage was added to the bone block procedure to prevent engagement. Patients with bone loss less than 20%, multidirectional instability, rotator cuff tear, generalised ligamentous laxity, glenohumeral arthritis, fracture-dislocation, prior shoulder surgery, failed previous stabilization procedure, and associated neurological pathology were excluded from the study.
This retrospective cohort study was conducted after obtaining approval from the institutional ethics committee, and all procedures were performed in accordance with the ethical standards laid down in the Declaration of Helsinki. Demographic data including age, sex, side involved, dominance, number of instability episodes, mechanism of injury, and duration of symptoms were collected from hospital records. The indication for surgery was based on recurrent symptomatic instability associated with critical glenoid bone loss, with or without a concomitant Hill–Sachs lesion.
Glenoid and humeral bone defects were quantified using pre-operative CT scans with the best fit circle method. Three-dimensional computed tomography images were reviewed to accurately assess the extent of glenoid bone loss and to classify the Hill–Sachs lesion according to the glenoid track concept as on-track or off-track. The decision to add remplissage was made pre-operatively based on imaging findings and confirmed intra-operatively by assessing engagement in the functional position of abduction and external rotation.
All operations were performed by the same team of surgeons. The arthroscopic Eden–Hybinette procedure was performed using a standardized surgical technique. Adequate graft positioning, flush alignment with the native glenoid surface, and restoration of the glenoid arc were ensured under arthroscopic visualization. When indicated, remplissage was performed by tenodesis of the posterior capsule and infraspinatus tendon into the Hill–Sachs defect.
The patients were followed-up post-operatively according to a standardized protocol. Postoperative rehabilitation was uniform for all patients and included initial immobilization in a sling, followed by progressive passive and active-assisted range-of-motion exercises, and subsequent strengthening exercises. Return to sports and heavy activities was permitted based on clinical recovery and functional assessment.
Clinical assessment was done using the WOSI (Western Ontario Shoulder Instability) index and the Rowe scores pre-operatively and post-operatively at 3 months, 6 months, 12 months and 2 years. These validated outcome measures were used to assess pain, function, stability, and quality of life. Complications such as recurrent instability, graft-related problems, infection, and stiffness were documented.
The follow-up protocol involved clinical examinations using the apprehension, Jobe’s relocation, and load-and-shift tests to assess shoulder stability and rule out laxity. Range of motion (ROM) was evaluated for both active and passive movements in flexion, abduction, and internal/external rotation at 0° and 90° abduction. Comparisons were made with the contralateral shoulder where appropriate to identify any clinically significant restriction, particularly loss of external rotation. Recurrence of instability was defined as any episode of dislocation or symptomatic subluxation during the follow-up period.
Surgical technique
All patients underwent an arthroscopic Bone Block Cerclage procedure for anterior shoulder instability with glenoid bone loss. Four patients with engaging Hill-Sachs lesions underwent concomitant remplissage. The patient is positioned in the beach-chair position. The shoulder and arm are prepared and draped in the standard sterile fashion. Diagnostic arthroscopy is performed through a posterior portal to assess the extent of glenoid bone loss and to confirm the presence of any capsulo-labral deficiency. A tricortical iliac crest autograft of desired size, is harvested using osteotomes, maintaining the concavity of the inner table to match the contour of the glenoid articular surface. A standard anterior portal is established to allow instrument access for debridement and graft placement. The glenoid defect is prepared to obtain a flat, bleeding surface to promote graft healing. An accessory posterior portal is made to pass the glenoid guide jig [figure 1]. The glenoid guide is then introduced through the posterior portal. Under direct visualization, the guide sleeve is positioned on the glenoid face, ensuring that the planned tunnel exits at the centre of the anterior defect. Two parallel guide pins are then drilled from posterior to anterior through the glenoid, spaced appropriately to match the graft size. The drill is removed, and the cerclage passing wires or polypropylene threads are advanced through the tunnels. The bone block - iliac crest autograft - is trimmed to the desired dimensions and predrilled to match the spacing of the glenoid tunnels [Figure 2]. Two high-strength cerclage sutures are loaded into the passing wires and shuttled from posterior to anterior [Figure 3]. The tapes are retrieved through the anterior portal. The bone block is attached to the cerclage tapes and gently introduced through the anterior portal [Figure 4]. Using the tapes as guides, the graft is advanced into position against the anterior glenoid defect. Once seated flush with the native articular surface, the cerclage tapes are tensioned sequentially using the cerclage tensioner device. This step compresses the graft uniformly against the glenoid rim, providing strong fixation without the need for metal screws. The tension is maintained as the locking mechanism is engaged, and the excess tape is cut flush to the bone. The technique sought a flush graft-to-glenoid articular surface and restoration of the glenoid arc. Final arthroscopic inspection confirms the graft’s position and stability [Figure 5]. The glenoid contour is restored, and the construct demonstrated excellent compression and alignment. The capsulo-labral tissue is repaired to the graft using suture anchors to re-establish the soft-tissue restraint. The shoulder is taken through a full range of motion to confirm construct stability. The portals are closed in standard fashion, and a sterile dressing is applied. Post-operatively, the patient is placed in a sling for protection, and a structured rehabilitation program is initiated to restore motion and strength gradually - passive abduction and forward flexion to 90 degrees started on day one, pendulum exercises at four weeks, active range of motion exercises at six weeks and weight training at three months. The bone block cerclage technique offers stable fixation, facilitates graft incorporation, and eliminates hardware-related complications.
Statistical analysis
Statistical analysis was performed using SPSS software version 29. The Mann–Whitney test was applied for nonparametric data, while unpaired t-tests were used for parametric data. The Pearson correlation coefficient was calculated wherever applicable. A p-value of < 0.05 was considered statistically significant.
Results
Among the 18 patients there were 14 males (78%) and 4 females. The dominant side was affected in 13 cases (72%) and the non-dominant side in 5 cases. The mean age of the patients in this series was 33 years and 6 months. The mean number of dislocations before the surgery was 4.1. The mean time period between initial dislocation and surgery was 4.6 years. The mean duration of surgery was eighty minutes. The average length of hospital stay was 2.5 days. The average follow-up period in this series was 38 months, the longest follow-up being 7 years and shortest being 6 months. There were no immediate post-operative complications. Two patients developed superficial surgical-site infections which settled with oral antibiotics, four patients reported donor-site sensory disturbances at the iliac crest. No cases of re-dislocation were noted. One patient had a single subluxation episode at two years which required rehabilitation alone and did not recur.
Functional outcome
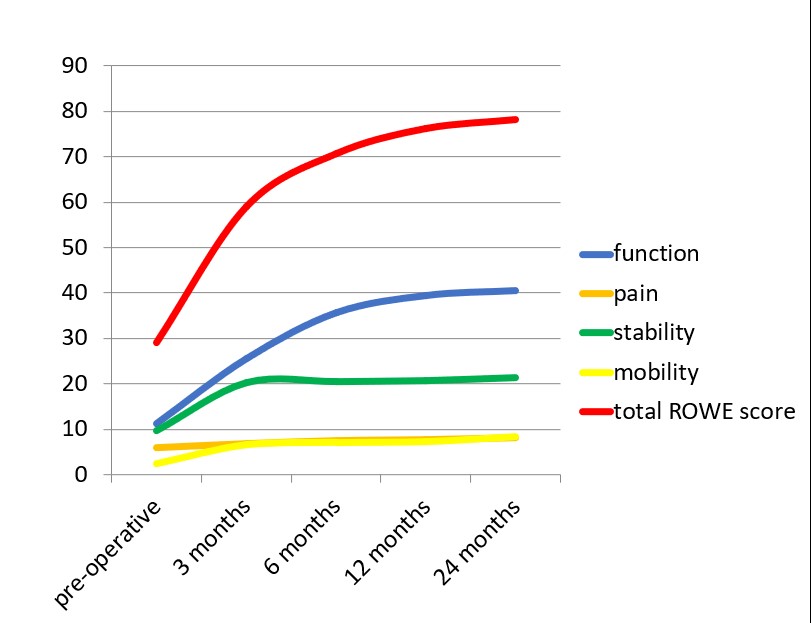
The modified Rowe score improved from 29.16 ± 14.1 (pre-operative) to 78.25 ± 14.23 at 24 months, ranging from 65 to 100, a significant improvement of 169% (p<0.001) [Figure 6]. The mean pre-operative functional, pain, stability and mobility scores were 12.24, 6.82, 10.52 and 2.5 respectively. At final follow-up the mean scores improved to 40.5, 8.16, 22.25 and 8.53 respectively. The results based on the modified ROWE score are presented as Mean ± Standard Deviation, and statistical comparison between pre-operative and postoperative groups was performed using the paired t-test [Table 1]. There was no significant relationship between the age of patients and the number of dislocations (r=- 0.12; p=0.72). There was no significant correlation of age of patient (r=0.16; p=0.11) or the number of prior dislocations (r=-0.08; p=0.19) with the final Rowe score.
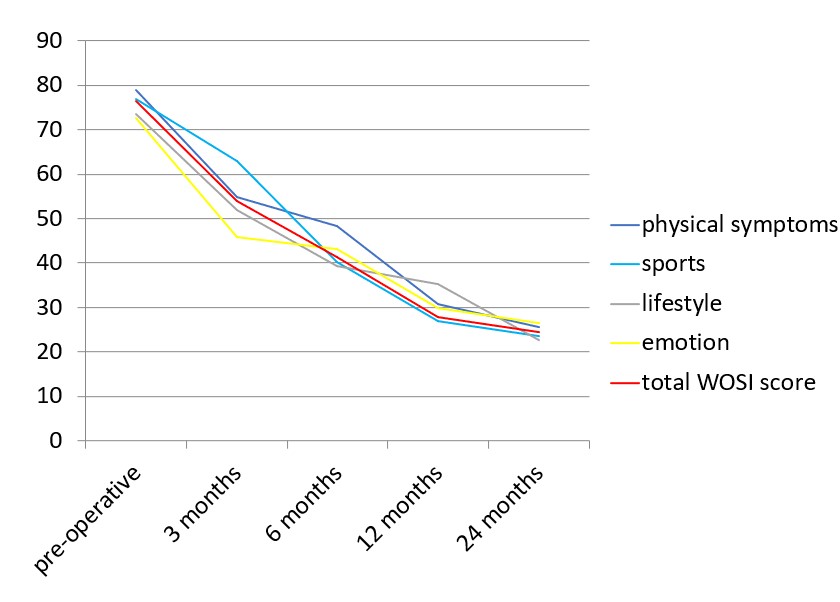
The WOSI index improved from 76.52 ± 3.62 (pre-operative) to 24.56 ± 4.53 at 24 months ranging from 17.5 to 27.5 (p<0.001) [Figure 7]. The mean pre-operative physical symptoms, sports, life style and emotion scores were 78.99,76.99, 73.5 and 72.75 respectively. At final follow-up the mean scores improved to 40.5,8.16, 21.25, 8.33 respectively. The results for the individual parameters of the WOSI score are presented as Mean ± Standard Deviation, and statistical comparison between preoperative and postoperative values using the paired t-test revealed significant differences across all domains [Table 2]. There was no significant relationship of age of patient (r=0.23; p=0.18) or the number of previous dislocations (r=0.16; p=0.27) with the final WOSI score. The mean post-operative Rowe score was inversely correlated with the mean post-operative WOSI score (r = −0.66).
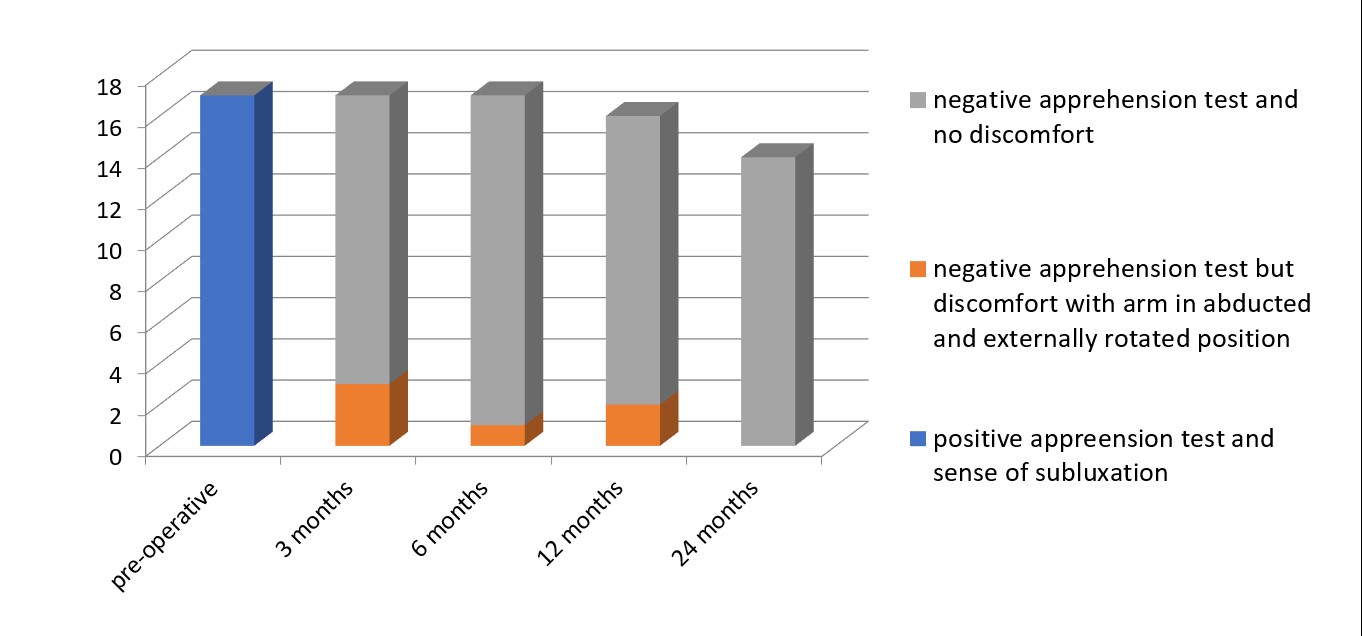
Stability was defined by a negative apprehension sign and good functional range of motion. All 18 patients had positive apprehension test and a sense of subluxation pre-operatively. At three months 14 patients had negative apprehension test, 4 patients had negative apprehension test but some discomfort when the arm was placed in abducted and externally rotated position and none had a positive apprehension test. At six months 16 patients had negative apprehension test, 2 patients had negative apprehension test but some discomfort when the arm was placed in abducted and externally rotated position and none had a positive apprehension test. At twelve months 15 patients had negative apprehension test, 2 patients had negative apprehension test but some discomfort when the arm was placed in abducted and externally rotated position and none had a positive apprehension test. At two years all 15 patients completing follow-up had negative apprehension test [Figure 8]. There was significant improvement in mobility with 14 patients regaining normal range of motion and 4 patients in whom remplissage was added having a loss of external rotation of less than 25 degrees.
Discussion
High energy traumatic shoulder dislocation can result in significant glenohumeral bone deficiency leading to subsequent multiple low energy or spontaneous events. Also, recurrent shoulder instability may lead to erosion or impaction resulting in bone loss. Burkhart et al. [6], in a case series involving 194 consecutive arthroscopic Bankart repairs performed using the suture anchor technique, observed that significant bone defects were present in 66.67% of patients with recurrent shoulder instability - either as an inverted pear-shaped glenoid or an engaging Hill-Sachs lesion. They concluded that arthroscopic Bankart repair yields optimal outcomes in patients without substantial bone loss. On reviewing the literature, bony Bankart lesions are present in approximately 20% of first-time shoulder dislocations and in up to 90% of recurrent dislocations [7]. Hill-Sachs lesions are observed in nearly 100% of patients with recurrent dislocations, compared to about 67% in those experiencing a first-time dislocation [8,9,10]. In our study four patients with engaging Hill-Sachs lesions underwent concomitant remplissage.
The Eden-Hybinette procedure, first described in 1932, involved the use of an L-shaped iliac crest bone graft placed between the anterior glenoid and its periosteum, with a small portion of the graft intentionally overhanging the anterior glenoid margin and without any fixation. De Palma later modified the technique by introducing screw fixation to achieve stable graft consolidation [11].
This case series demonstrates that arthroscopic Eden–Hybinette with iliac crest bone graft can restore stability and function in patients with critical glenoid bone loss. Over a mean follow-up of 38 months, there were no re-dislocations and only one episode of subluxation, suggesting the procedure reliably restored stability in this cohort. This aligns with other reports of free bone-block procedures showing low recurrence when graft positioning and fixation are adequate. Significant, clinically meaningful improvements in both modified Rowe and WOSI scores were seen. Tahir M et al, in their systematic review of clinical and radiological outcomes concluded that arthroscopic bone block stabilisation is associated with high rates of graft union, significant improvements in the WOSI and Rowe scores, and a low rate of complications, including re-dislocation in the short to mid-term [12]. Sayegh T E et al have observed similar results in their systematic review of bone block procedures for recurrent anterior shoulder instability, using allografts [13]. In our series, the modified ROWE score and WOSI scores revealed excellent to good functional outcome. The total ROWE score improved by 168% while the total WOSI index ameliorated by 67.9% following the Eden-Hybinette procedure. Both the objective scoring criteria were inversely correlated. Lunn et al [14], demonstrated objective good to excellent outcomes as per the modified ROWE scoring in 82% of patients with 12% rate of re-dislocation and 6% rate of recurrent dislocation. In our study none of the patients had re-dislocation. Hazra S et al, have reported similar results in their case series including patients undergoing open or arthroscopic Eden-Hybinette procedure for recurrent instability after an index procedure [15]. Majority (77.78%) of the patients in our series regained normal ROM. The limited loss of less than 25 degrees in a minority, when remplissage was added, is an important consideration when compared to coracoid transfer techniques which may impose greater external rotation loss. Iliac crest bone graft offers cancellous bone favourable for incorporation. The operative time in our series (80 min) is shorter than most Latarjet series [16], and revision to Latarjet remains possible if needed. In this series, the use of cerclage tape fixation appears to provide stable fixation with low hardware-related morbidity, though longer-term radiographic graft incorporation data would strengthen this conclusion. Donor-site sensory disturbances in four and superficial infections in two cases were the principal complications. Donor-site morbidity remains a consideration when harvesting Iliac crest bone graft and should be discussed during consent. Additionally, subtle pre-operative glenohumeral arthritis should be carefully excluded thorough clinical evaluation and appropriate investigations.
Conclusion
Arthroscopic Eden–Hybinette procedure using an iliac crest autograft is an effective option for managing recurrent anterior shoulder instability with critical (≥20%) glenoid bone loss. In this series of 18 patients, the procedure resulted in significant and clinically meaningful improvements in shoulder stability and functional outcomes at mid-term follow-up, with a low rate of recurrence and acceptable complications. Restoration of the glenoid arc allowed conversion of off-track Hill–Sachs lesions to on-track lesions while preserving shoulder range of motion in most patients. Arthroscopic Eden–Hybinette represents a reliable alternative to coracoid transfer procedures in selected patients, particularly when preservation of the coracoid is desired. Further prospective studies with larger cohorts and longer follow-up are warranted to confirm these findings.
Limitations
This study presents the mid-term outcomes of a bony augmentation technique based on a retrospective analysis. The sample size is relatively small given the study duration, as this procedure is infrequently performed as a primary surgical option for recurrent shoulder dislocations. Larger cohorts and longer follow-up periods are needed to better assess potential complications and their impact on clinical outcomes, quality of life, and functional activities. Additionally, this study did not assess radiographic parameters such as graft union or resorption.
Funding: No funding was received for the study
Conflict of interest: None declared
Ethical Approval: The study was approved by the Institutional Ethics Committee. Informed consent was obtained from all subjects.
References
1. Balg F, Boileau P. The instability severity index score: a simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation. The Journal of bone and joint surgery. British volume. 2007 Nov;89(11):1470-7.
2. Tauber M, Resch H, Forstner R, Raffl M, Schauer J. Reasons for failure after surgical repair of anterior shoulder instability. Journal of shoulder and elbow surgery. 2004 May 1;13(3):279-85.
3. Tehrany AM, Parten PM. Quantifying glenoid bone loss arthroscopically in shoulder instability. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2002 May 1;18(5):488-91.
4. Jankauskas L, Rüdiger HA, Pfirrmann CW, Jost B, Gerber C. Loss of the sclerotic line of the glenoid on anteroposterior radiographs of the shoulder: a diagnostic sign for an osseous defect of the anterior glenoid rim. Journal of shoulder and elbow surgery. 2010 Jan 1;19(1):151-6.
5. Hovelius L, Sandström B, Olofsson A, Svensson O, Rahme H. The effect of capsular repair, bone block healing, and position on the results of the Bristow-Latarjet procedure (study III): long-term follow-up in 319 shoulders. Journal of shoulder and elbow surgery. 2012 May 1;21(5):647-60.
6. Burkhart SS, De Beer JF. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2000 Oct 1;16(7):677-94.
7. Taylor DC, Arciero RA. Pathologic changes associated with shoulder dislocations: arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. The American journal of sports medicine. 1997 May;25(3):306- 11.
8. Owens BD, Nelson BJ, Duffey ML, Mountcastle SB, Taylor DC, Cameron KL, Campbell S, DeBerardino TM. Patho anatomy of first-time, traumatic, anterior glenohumeral subluxation events. JBJS. 2010 Jul 7;92(7):1605-11.
9. Griffith JF, Antonio GE, Yung PS, Wong EM, Yu AB, Ahuja AT, Chan KM. Prevalence, pattern, and spectrum of glenoid bone loss in anterior shoulder dislocation: CT analysis of 218 patients. American Journal of Roentgenology. 2008 May;190(5):1247-54.
10. Widjaja AB, Tran A, Bailey M, Proper S. Correlation between Bankart and Hill‐Sachs lesions in anterior shoulder dislocation. ANZ journal of surgery. 2006 Jun;76(6):436-8.
11. De Palma AF. In: Surgery of the shoulder, Vol 1. Philadelphia, PA: JB Lippincott; 1983. p. 532-4.
12. Tahir M, et al. Arthroscopic bone block stabilization procedures for glenoid bone loss in anterior glenoid instability: A systematic review of clinical and radiological outcomes. OrthopTraumatolSurg Res. 2021.
13. Sayegh ET, et al. Allograft reconstruction for glenoid bone loss in glenohumeral instability: a systematic review. Arthroscopy. 2014.
14. JV, Castellano-Rosa J, Walch G. Recurrent anterior dislocation after the Latarjet procedure: outcome after revision using a modified Eden-Hybinette operation. Journal of shoulder and elbow surgery. 2008 Sep 1;17(5):744-50.
15. Hazra S, Chandra M, Saha R, Dutta S. Functional outcome assessment of Eden-Hybinette procedure for recurrent shoulder dislocation: a prospective study evaluating Modified Rowe and WOSI scores.
16. Berte Boe, Ragnhild Oydna Støen, Ingvild Blich, Gilbert Moatshe, Tom Clement Ludvigsen. Learning Curve for Arthroscopic Shoulder Latarjet Procedure Shows Shorter Operating Time and Fewer Complications with Experience. Arthroscopy: The Journal of Arthroscopic & Related Surgery, Volume 38, Issue 8,2022