A RARE CASE OF CHRONIC CAUDA EQUINA SYNDROME SECONDARY TO HIGH-GRADE DYSPLASTIC SPONDYLOLISTHESIS IN A YOUNG ADULT
INTRODUCTION
Cauda equina syndrome (CES) is a serious neurological condition occurring due to compression or injury to cauda equina. It cause motor, sensory and autonomic dysfunction like saddle anesthesia,1bowel, bladder incontinence and lower limb weakness. The causes are disc herniation, spinal stenosis, trauma, neoplasm and spondylolisthesis.
Spondylolisthesis is forward slippage of a vertebra relative to the one below it. Dysplastic spondylolisthesis is a developmental subtype, due to congenital anomalies of the lumbosacral junction like hypoplasia of facets, domed sacrum, and dysplasia of pars interarticularis.2High-grade-Meyerding grade III,IV & V, the deformity can cause biomechanical stress, sagittal imbalance, and predisposition to neurological compromise.
High-grade dysplastic spondylolisthesis is uncommon. History include progression of slip, increasing deformity, and secondary structural changes that increase the risk of neural element compression. Many patients present with back pain, radicular symptoms, postural changes, and difficulty walking.3
As chronic compression of the nerve roots in CES can lead to irreversible damage, early recognition, imaging, and surgical decompression are essential to optimize outcomes. Among young adults, with high-grade dysplastic deformity, slow progression may mask the severity until major symptoms appear. The present case shows an unusual presentation of chronic CES secondary to high-grade dysplastic spondylolisthesis in a young adult, showing diagnostic and therapeutic challenges.
A 21-year-old female presented with a 2-year history of chronic low back pain, which was continuous in nature and radiated to both lower limb, more on the left side. The pain was associated with bilateral lower limb numbness, paresthesia and weakness, leading to progressive difficulty in walking. She also reported neurogenic claudication, with perineal and perianal region saddle anesthesis.
There was a history of urinary incontinence and recurrent urinary tract infections for the past 2 years, suggestive of autonomic involvement. The patient complained of constipation, indicating chronic sacral nerve root compromise.
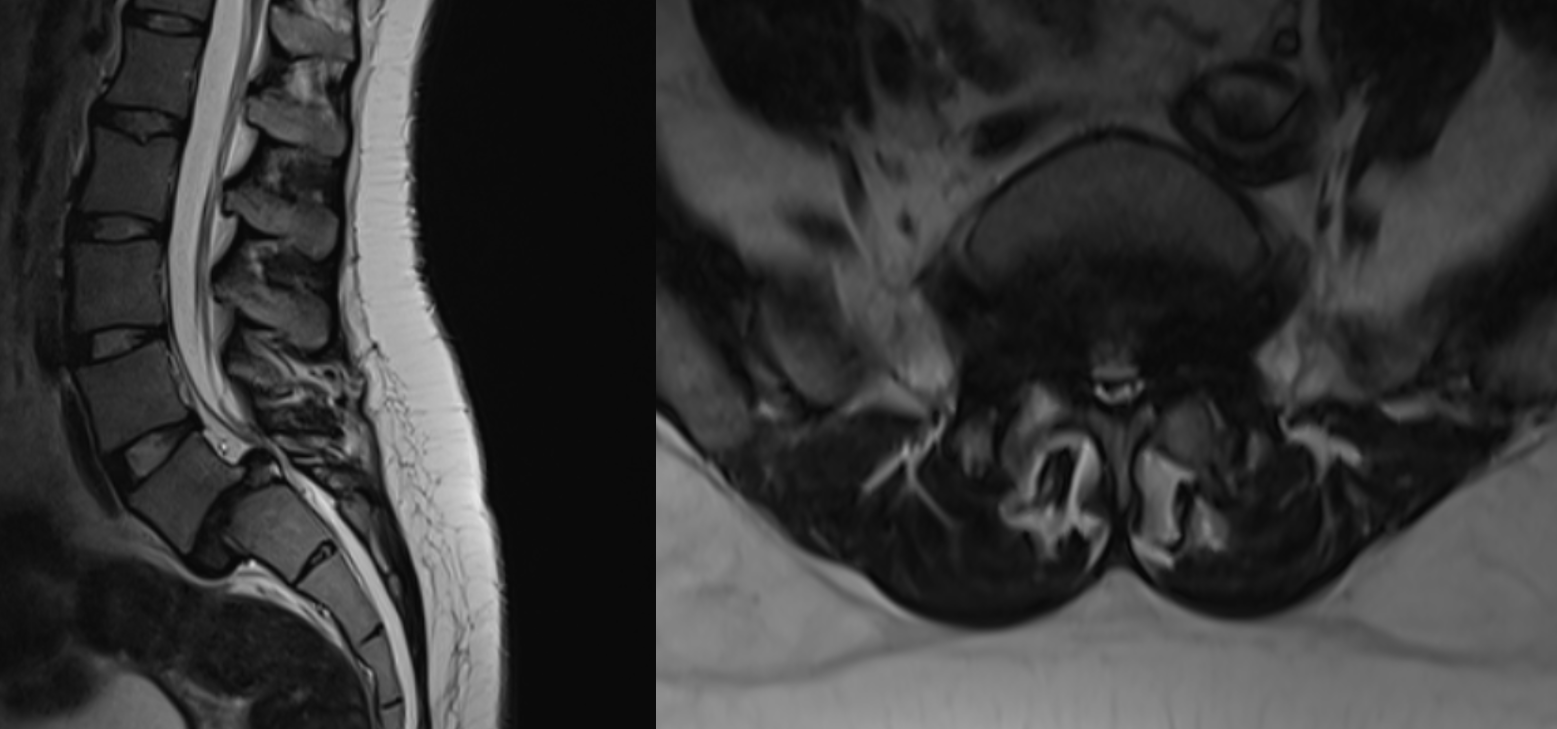
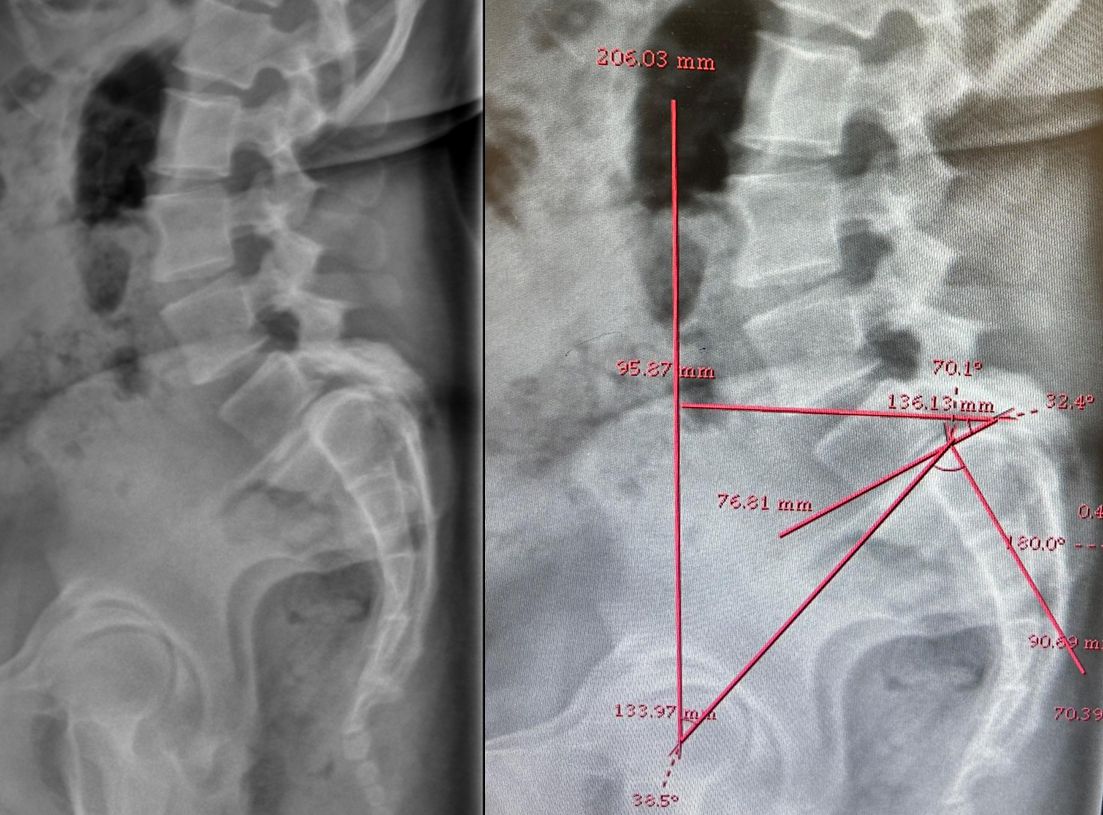
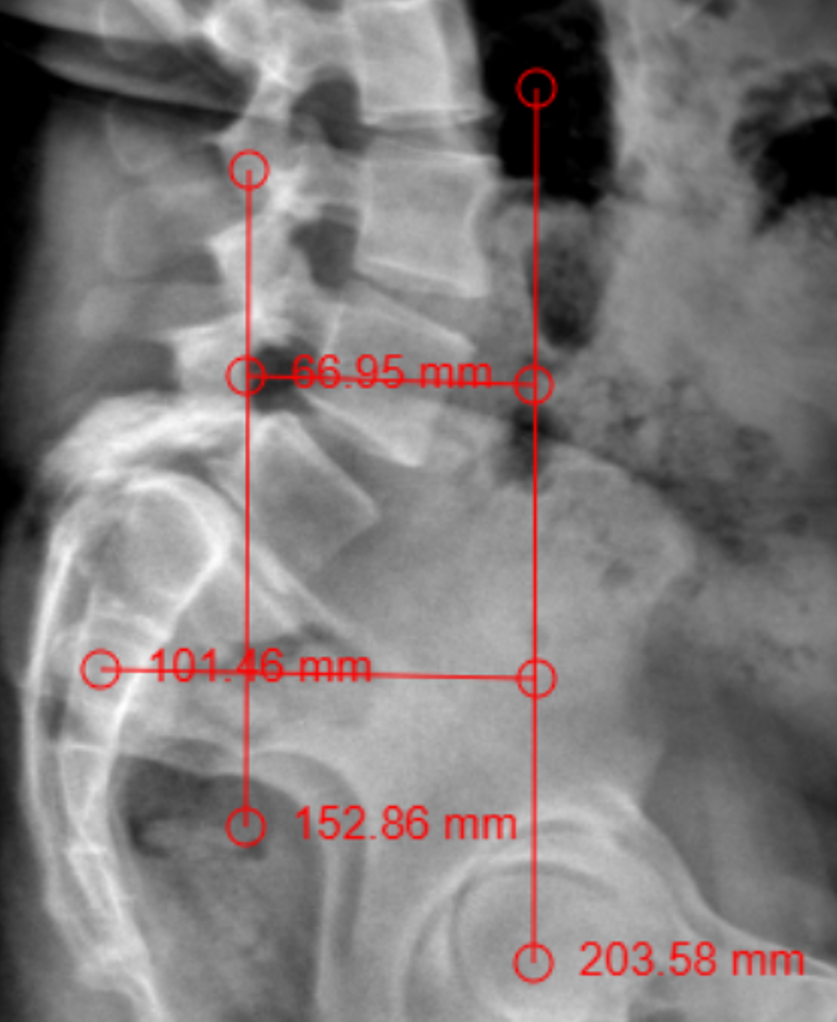
The patient had lumbar spine tenderness localized over the L4 and L5 vertebral levels. Lumbar spine range of motion (ROM) is painful on flexion and extension. Neurological examination showed positive Lasegue’s test at 40° on the right and 30° on left. Motor examination (5/5) in L1, L2, and L3 myotome bilaterally, with reduced power (4/5) in the L4, L5, and S1 myotome on both sides. Sensory examination showed normal sensation in the L1, L2, and L3 dermatomes, reduced sensation on the left at L4, and reduced sensation bilaterally at L5 and S1 S2 S3 S4 S5. Reflex examination showed diminished knee and ankle reflexes and plantar was mute on both side. MRI of lumbar spine with whole spine screening showed anterior listhesis of L5 over S1,central disc bulge,hypertrophy of the facet joints and ligamentum flavum caused severe central canal stenosis, lateral recess narrowing, compression of cauda equina roots, and severe bilateral foraminal stenosis with impingement of the exiting L4 nerve roots bilaterally (Figure1). Post-void residual urine volume is 232 cc on ultrasonography. Diagnosis was high dysplastic spondylolisthesis of L5 over S1, Meyerding Grade III, SDSG – Type 5 balance spine retroverted pelvics based on pelvic incidence 70o pelvic tilt 38osacral slope 32o (Figure 2). The high dysplastic according to the severity index.The patient was counseled on the need for immediate surgical decompression and lumbosacral stabilization to stop neurological deterioration. The recovery of bladder and bowel function was explained to be guarded due to the chronicity of symptoms. After getting informed and written consent the patient underwent posterior decompression and spondylolisthesis reduction with stabilization from L4 to S1, along with bilateral posterolateral fusion at L4-L5-S1 and posterior interbody fusion at L5-S1 under general anesthesia.We fixed L4 also, as the current case is an unstable zone.This zone was identified using a standing lateral radiograph of the lumbar spine that also captures the hips.On radiograph, square area is demarcated by drawing a horizontal line through the center of the S2 vertebral body. The boundaries of the line segment are determined by two vertical reference lines: one is the gravity line, which runs vertically through the midpoint of the inferior endplate of L5, and the other represents the ground reaction force, passing vertically through the center of the femoral head (Figure 3).
DISCUSSION
High-grade dysplastic spondylolisthesis is a rare but important cause of spinal instability and neurological compromise, usually at lumbosacral junction. Dysplastic morphology like domed sacrum, abnormal facets, and elongation of neural arch structures predisposes to severe vertebral slip, canal compromise, and nerve root compression.5 When the slip progresses to Grade IV or spondyloptosis, cauda equina compression can occur. This causes sensory, motor, and autonomic dysfunction. Chronicity of compression is main determinant of prognosis. Long-standing neural compromise reduces chance of full recovery, particularly of bladder and bowel function.
Surgical strategies are: in situ fusion, partial reduction, or complete reduction with circumferential fusion. Reduction with fusion is associated with better restoration of spinopelvic balance and long-term outcomes, but it carries the risk of neurological injury due to nerve stretch. Complete reduction and circumferential fusion in children and adolescents helps to achieve substantial deformity correction and high fusion rates with improvement in functional outcomes. But autonomic recovery is unpredictable.7
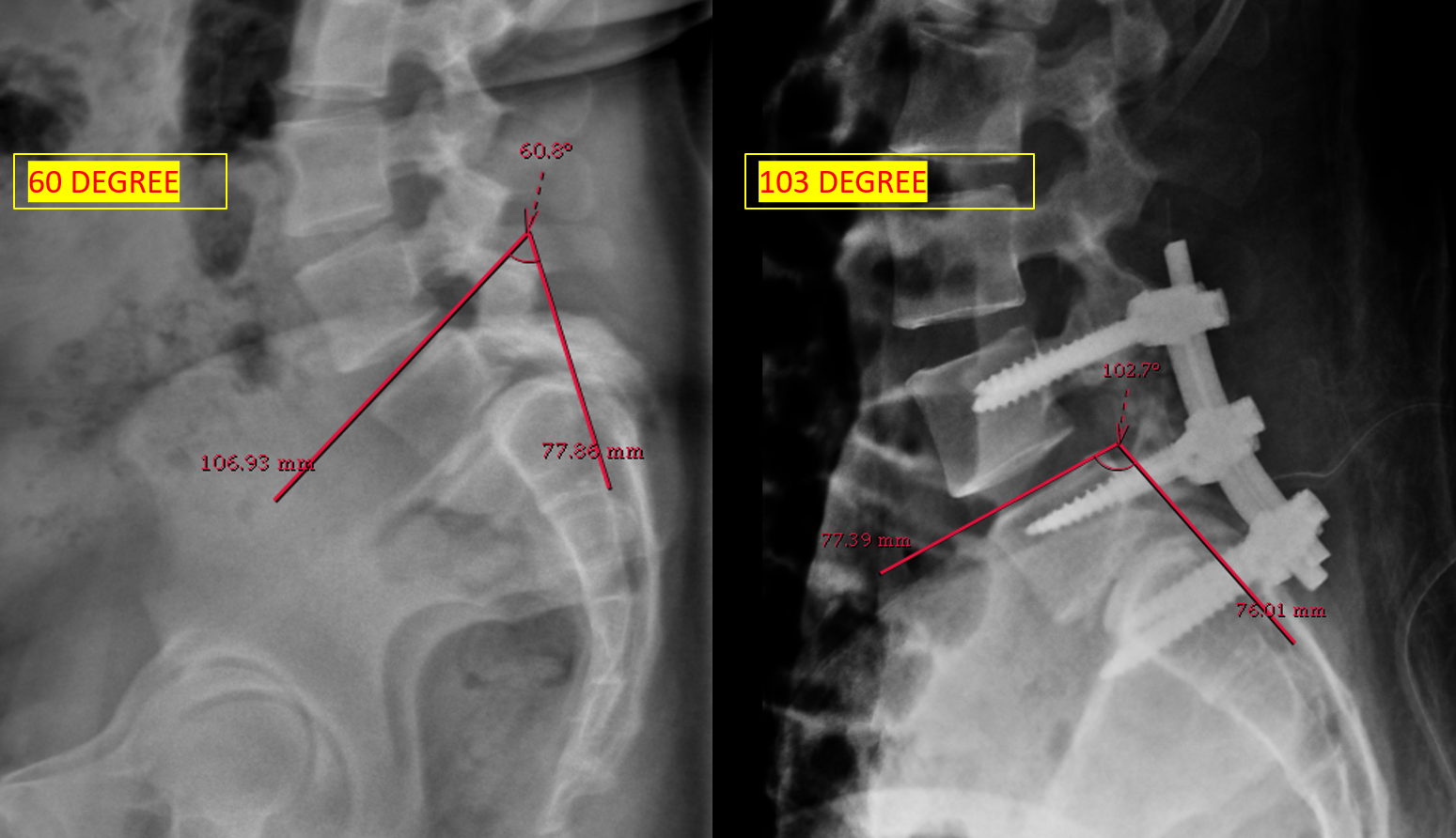
Surgical planning was done in the current study, as per the model described by Lamartina. That model provides practical tool for preoperative planning and supports the surgical decision to extend fixation above the L5–S1 segment.8post op lumbosacral kyphosis improved (Figure 4)
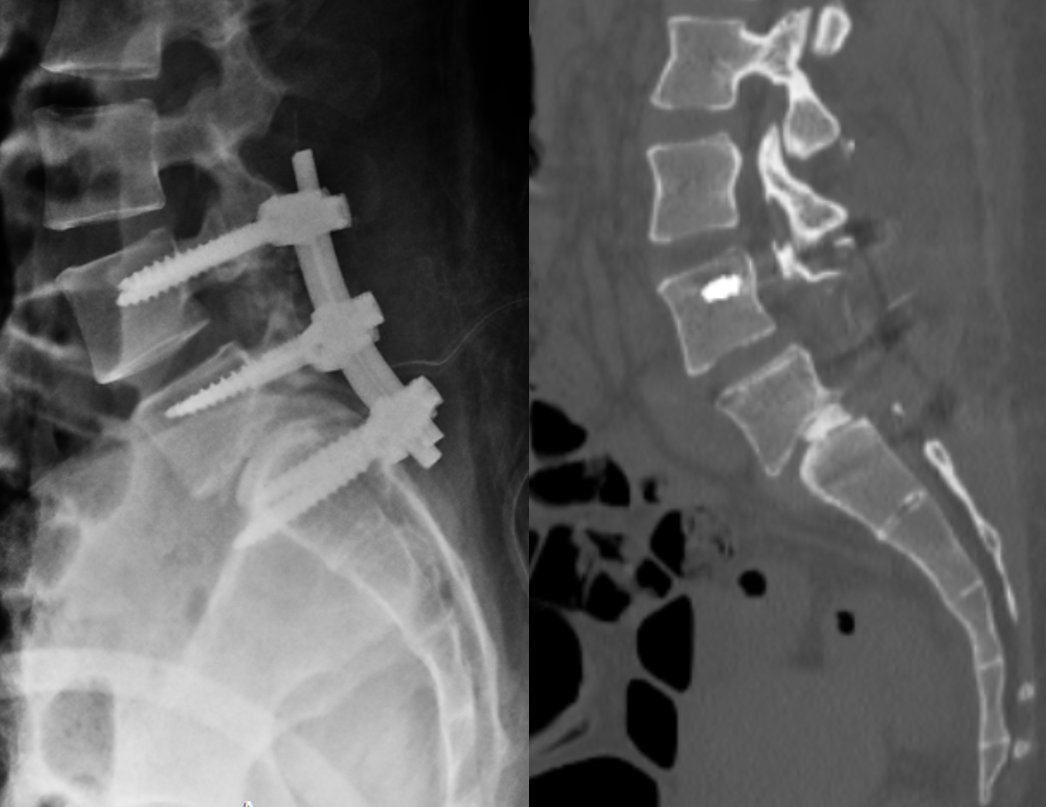
The literature also showed that long-standing cases, as in this patient with a two-year history of symptoms, have guarded prognosis for sphincter recovery. Pain relief, motor improvement, and functional ambulation are achievable after decompression and stabilization with pedicle screw, connecting rod and autologous bone graft (Figure 5).9 Case reports and prospective studies showed that urinary and bowel dysfunction may improve gradually after surgery, but complete recovery is not always possible. So, Surgical decompression and stabilization are standard of care to prevent further deterioration, but chronicity of symptoms must be taken into account when counseling patients regarding outcomes.
Emary PC.10 Case reports of high-grade spondylolisthesis have been rarely published in the chiropractic literature. Documented here is a case involving a 28-year-old woman who presented to the World Spine Care clinic in the Dominican Republic with minimal neuromusculoskeletal symptoms despite a grade 4 spondylolytic spondylolisthesis. The key imaging and etiological features of this clinical disorder are presented.
CONCLUSION
Chronic cauda equina syndrome secondary to high-grade dysplastic spondylolisthesis in young adults is an uncommon. Early recognition and timely surgical management are important prevent irreversible sequelae, as delayed presentation limits the chance of full neurological recovery. This case proves the importance of more clinical suspicion, comprehensive neurological evaluation, and multidisciplinary intervention in young patients presenting with persistent low back pain and progressive neurological symptoms.
REFERENCES
- Spector LR, Madigan L, Rhyne A, Darden B 2nd, Kim D. Cauda equina syndrome. J Am Acad Orthop Surg. 2008;16(8):471–9. doi:10.5435/00124635-200808000-00006. PMID:18664636.
- Fu KM, Smith JS, Polly DW Jr, Perra JH, Sansur CA, Berven SH, et al. Morbidity and mortality in the surgical treatment of six hundred five pediatric patients with isthmic or dysplastic spondylolisthesis. Spine (Phila Pa 1976). 2011;36(4):308–12. doi:10.1097/BRS.0b013e3181cf3a1d. PMID:20739916.
- Ploumis A, Hantzidis P, Dimitriou C. High-grade dysplastic spondylolisthesis and spondyloptosis: report of three cases with surgical treatment and review of the literature. Acta Orthop Belg. 2005;71(6):750–7. PMID:16459872.
- Kasliwal MK, Smith JS, Shaffrey CI, Saulle D, Lenke LG, Polly DW Jr, et al. Short-term complications associated with surgery for high-grade spondylolisthesis in adults and pediatric patients: a report from the scoliosis research society morbidity and mortality database. Neurosurgery. 2012;71(1):109–16. doi:10.1227/NEU.0b013e3182535881. PMID:22407074.
- Sudarshan PK, Suthar HR, Varma VK, Krishnan A, Hegde SK. Long-term experience with reduction technique in high-grade spondylolisthesis in the young. Int J Spine Surg. 2018;12(3):399–407. doi:10.14444/5047. PMID:30276098; PMCID:PMC6159655.
- Jones-Quaidoo SM, Hunt T, Shaffrey CI, Arlet V. Return of normal urological and neurological function after revision surgery for spondyloptosis: case report. J Neurosurg Spine. 2007;6(3):272–5. doi:10.3171/spi.2007.6.3.272. PMID:17355027.
- Kanematsu R, Hanakita J, Takahashi T, Minami M, Inoue T, Miyasaka K, et al. Improvement in neurogenic bowel and bladder dysfunction following posterior decompression surgery for cauda equina syndrome: a prospective cohort study. Neurospine. 2021;18(4):847–53. doi:10.14245/ns.2142252.126. PMID:35000340; PMCID:PMC8752717.
- Lamartina C, Zavatsky JM, Petruzzi M, Specchia N. Novel concepts in the evaluation and treatment of high-dysplastic spondylolisthesis. Eur Spine J. 2009;18(Suppl 1):S133–S142.
- Kunze KN, Lilly DT, Khan JM, Louie PK, Ferguson J, Basques BA, et al. High-grade spondylolisthesis in adults: current concepts in evaluation and management. Int J Spine Surg. 2020;14(3):327–40. doi:10.14444/7044. PMID:32699755; PMCID:PMC7343250.
- Emary PC, Eberspaecher SA, Taylor JA. High-grade spondylolytic spondylolisthesis. J Can Chiropr Assoc. 2017;61(2):162–6. PMID:28928499; PMCID:PMC5596974.