Study title
Beyond the Ankle Fracture: Understanding the Complex Challenges of Diabetic Ankle Fractures
Abstract
Ankle fractures in patients with diabetes represent a complex and high-risk subset of orthopaedic injuries, influenced by systemic and local disease factors. Diabetes, particularly when complicated by neuropathy, peripheral vascular disease, or chronic kidney disease, impairs bone metabolism and fracture healing. Furthermore, diabetic patients are predisposed to impaired wound healing, infection, and Charcot neuroarthropathy, which collectively complicate both operative and nonoperative management. Evaluation of diabetic ankle fractures requires comprehensive assessment of comorbidities, neurovascular status, and glycaemic control to stratify risk and guide management. Nonoperative strategies, including prolonged immobilisation and strict non-weightbearing, are associated with high complication rates, particularly in displaced or unstable fractures, and may contribute to malunion or development of Charcot arthropathy. Contemporary management favours operative intervention for unstable fractures, often employing augmented fixation strategies such as “ORIF plus” to optimize mechanical stability while preserving soft tissue integrity. Locking plates, multiple syndesmotic screws, minimally invasive techniques, and, in complex cases, primary tibio-talo-calcaneal arthrodesis are increasingly used to improve outcomes. Diabetic ankle fractures carry substantial risks of complications, including infection, impaired fracture healing, Charcot joint formation, and, in severe cases, amputation. These risks are heightened in patients with complicated diabetes, emphasizing the need for individualized, multidisciplinary management. Strategies such as the “rule of two” (doubling fixation, non-weightbearing duration, and follow-up frequency) are frequently applied to mitigate adverse outcomes. This review synthesizes current understanding of the pathophysiology, clinical evaluation, management strategies, and complications associated with diabetic ankle fractures. It underscores the importance of meticulous preoperative planning, patient-specific surgical approaches, and vigilant postoperative care to optimize fracture healing and improve overall patient outcomes. Recognition of the unique challenges posed by diabetes is essential to ensure safe, effective, and evidence-based care in this high-risk population.
- Introduction
Ankle fractures are among the most commonly encountered orthopaedic injuries, comprising approximately 9% of all fractures, with their incidence increasing in the elderly population in parallel with rising life expectancy.1,2 A Finnish predictive model has estimated a threefold increase in the incidence of ankle fractures by 2030, although the underlying reasons for this rise remain unclear.3 Diabetic patients constitute approximately 12% of all ankle fractures, and the management of this subgroup has attracted particular attention owing to its association with higher complication rates and increased overall healthcare costs.4 Diabetes is an escalating global epidemic and a leading contributor to both mortality and morbidity, significantly driving up healthcare costs worldwide.5 India ranks second in the world for the number of people with diabetes, with an estimated prevalence rate of 16.1 percent.6 Elevated blood glucose levels promote the increased production of advanced glycation end products, reactive oxygen species, and inflammatory mediators. Collectively, these factors enhance osteoclast activity while suppressing osteoblast function and bone formation, thereby increasing fracture risk and impairing fracture healing.7 Most of these patients also have concomitant comorbidities, including peripheral vascular disease and diabetic neuropathy, which further complicate the management of ankle fractures.8 Impaired wound healing and an increased risk of infection may influence the decision to pursue surgical treatment,9 whereas conservative management carries a risk of loss of reduction and delayed or impaired fracture union, potentially resulting in additional complications.10 Nonoperative management was associated with a 21-fold higher odds of complications compared with operative treatment.11 Moreover, both operative and non-operative treatment strategies in diabetic patients may increase the likelihood of developing Charcot neuroarthropathy, culminating in joint destruction, bone loss, and deformity.12,13 Patients with diabetes mellitus, especially those with diabetes-related comorbidities, may experience severe consequences following foot and ankle fractures. Notably, individuals with diabetes have been reported to carry a 7.4-fold higher risk of amputation after ankle fracture surgery compared with nondiabetic patients.14,15 This article provides an overview of ankle fractures in patients with diabetes, outlines the management strategies for this population, and further examines the associated complications.
- Impact of diabetes on bone tissue and physiology of fracture healing
Both type 1 and type 2 diabetes share key pathophysiological features affecting bone, including hyperglycaemia and increased production of advanced glycation end products (AGE), reactive oxygen species (ROS), and inflammatory mediators. Together, these factors enhance osteoclast activity, suppress osteoblast function and bone formation, thereby increasing fracture risk and impairing fracture healing.7 Hyperglycaemia adversely affects bone remodelling by altering osteoclast and osteoblast differentiation and by promoting a pro-inflammatory state through increased release of cytokines such as TNF-α, IL-1β, and IL-6. IL-6 enhances osteoclastogenesis and disrupts bone mineralisation. While excessive TNF-α promotes osteoclast activity and impairs fracture repair by reducing mesenchymal stem cell proliferation, inducing chondrocyte apoptosis, and inhibiting angiogenesis, resulting in cartilage resorption and impaired endochondral ossification.16–18 Hyperglycaemia also leads to the accumulation of AGE, which disrupt bone homeostasis by upregulating inflammatory cytokines and further driving osteoclastogenesis.7 In parallel, increased production of ROS induces oxidative stress, enhances RANKL-mediated osteoclast formation, and negatively impacts osteocytes and mesenchymal stem cells. Collectively, these mechanisms accelerate bone resorption and compromise overall bone health.18 Insulin exerts anabolic effects on bone through osteoblast insulin receptors and their substrates [Insulin Receptors (IRS-1 and IRS-2)] promoting osteoblast proliferation and bone homeostasis.19 Diabetes-associated peripheral vascular disease, vascular calcification, and impaired angiogenesis lead to tissue ischaemia and reduced delivery of oxygen and nutrients, thereby compromising wound and fracture healing.20 Loss of protective pain sensation from peripheral neuropathy results in an inability to perceive repetitive trauma, deep infection, ulceration, and wound complications.21
- Evaluation
Complicated diabetes is defined by the presence of end-organ damage, including neuropathy, peripheral arterial disease, and/or chronic kidney disease, and its differentiation is crucial as it significantly influences treatment decision-making, complication rates, and overall clinical outcomes.22 The initial assessment should include a detailed medical history, evaluation of diabetes-related complications, thorough neurovascular examination of the affected limb, adjunctive vascular assessment when pulses are not palpable, and review of baseline investigations, including relevant blood tests, to identify features of complicated diabetes.23
- Management of diabetic ankle fracture
Nonoperative management of ankle fractures involves closed contact casting with strict non-weightbearing until fracture union is confirmed. This is followed by a period of protected weight-bearing in a brace or boot for a further 2–3 months.24,25 In patients with diabetes, immobilisation may be required for up to three times longer than in nondiabetic patients to reduce the risk of malunion and Charcot arthropathy.26 Prolonged casting, however, increases the risk of cast-related ulceration and infection. Recognition of these complications is often delayed due to peripheral neuropathy.11 This treatment strategy requires strict patient compliance, close clinical observation, and serial radiological assessment to monitor skin integrity and detect early displacement. The treating surgeon should maintain a low threshold to abandon nonoperative care and proceed with surgical intervention if early complications or failure of conservative management are identified.24,25
Historically, operative management of ankle fractures in patients with diabetes was approached with caution.27 However, nonoperative treatment of unstable or displaced ankle fractures in this population has consistently been associated with unfavourable outcomes, leading most contemporary authors to advocate for open reduction and stable fixation. Lovy et al. reported a complication rate of approximately 75% following conservative management of displaced ankle fractures in diabetic patients, with higher incidences of malunion, loss of reduction, development of Charcot arthropathy, cast-related ulceration, deep infection, and unplanned surgical intervention compared with surgically treated cases.11 Similarly, Flynn et al. demonstrated increased infection rates among diabetic patients managed nonoperatively,28 while McCormack and Leith observed a high prevalence of malunion and loss of reduction following conservative treatment of displaced ankle fractures.27 This unacceptably high complication rate indicates that surgical fixation is justified to stabilise unstable fractures, despite the associated risk of perioperative complications.11
Guidelines from the British Orthopaedic Foot & Ankle Society do not support nonoperative casting for unstable ankle fractures in patients with diabetes. In cases of complicated diabetes, augmented fixation—commonly referred to as “open reduction and internal fixation (ORIF) plus”—is regarded as the preferred treatment strategy.29 The principles of ORIF plus include enhanced mechanical stability through the use of multiple syndesmotic screws, longer segment fixation, locking plate constructs, and, when indicated, transarticular pinning. Wukich et al. first described and categorised this approach in a comparative study of fixation methods, where ORIF plus emerged as the most commonly employed technique in diabetic patients.30 Importantly, it was associated with significantly lower complication rates than standard ORIF, despite being used more frequently in patients with complicated diabetes. Conversely, the addition of a supplementary external fixator to ORIF was associated with substantially higher complication rates. Collectively, these findings support the routine use of ORIF plus in diabetic ankle fractures, particularly in patients with complicated disease, over alternative fixation strategies.30
Schon et al. recommended that diabetic patients with peripheral neuropathy who sustain ankle fractures should be managed as Stage 0 Charcot neuroarthropathy, advocating prolonged non-weightbearing, augmented fixation, and extended immobilisation until clinical signs of inflammation have resolved.31 Prolonged immobilisation has traditionally been recommended to reduce complication rates in diabetic ankle fractures.32–34 However, emerging evidence has challenged this practice, proposing that early protected weight-bearing may help limit deconditioning and perioperative complications. Bazarov et al. reported a 25% complication rate in 48 surgically managed diabetic ankle fractures permitted protected weight-bearing at two weeks, which was lower than rates reported with conventional 6–8 weeks of non-weightbearing. Despite the limited sample size, these preliminary findings indicate a potential role for early weight-bearing in carefully selected patients; however, larger, methodologically robust studies are required to validate its safety, define appropriate selection criteria, and establish evidence-based protocols.35
Additional considerations include obesity and upper limb deconditioning, which are common in patients with diabetes and can make adherence to lower extremity weight-bearing restrictions difficult. Chiodo et al. reported that 27.5% of patients were non-compliant with postoperative non-weightbearing instructions, with nearly half of these patients experiencing an adverse event as a result. Consequently, meticulous discharge planning and postoperative care are essential in this high-risk population, and many patients may require additional support or supervised post-discharge placement to minimise non-compliance and associated complications.36 In summary, management is often guided by the “rule of two,” which emphasises doubling the degree of fixation, the duration of non-weightbearing, and the frequency of follow-up in patients with diabetic ankle fractures.
- Fixation choices
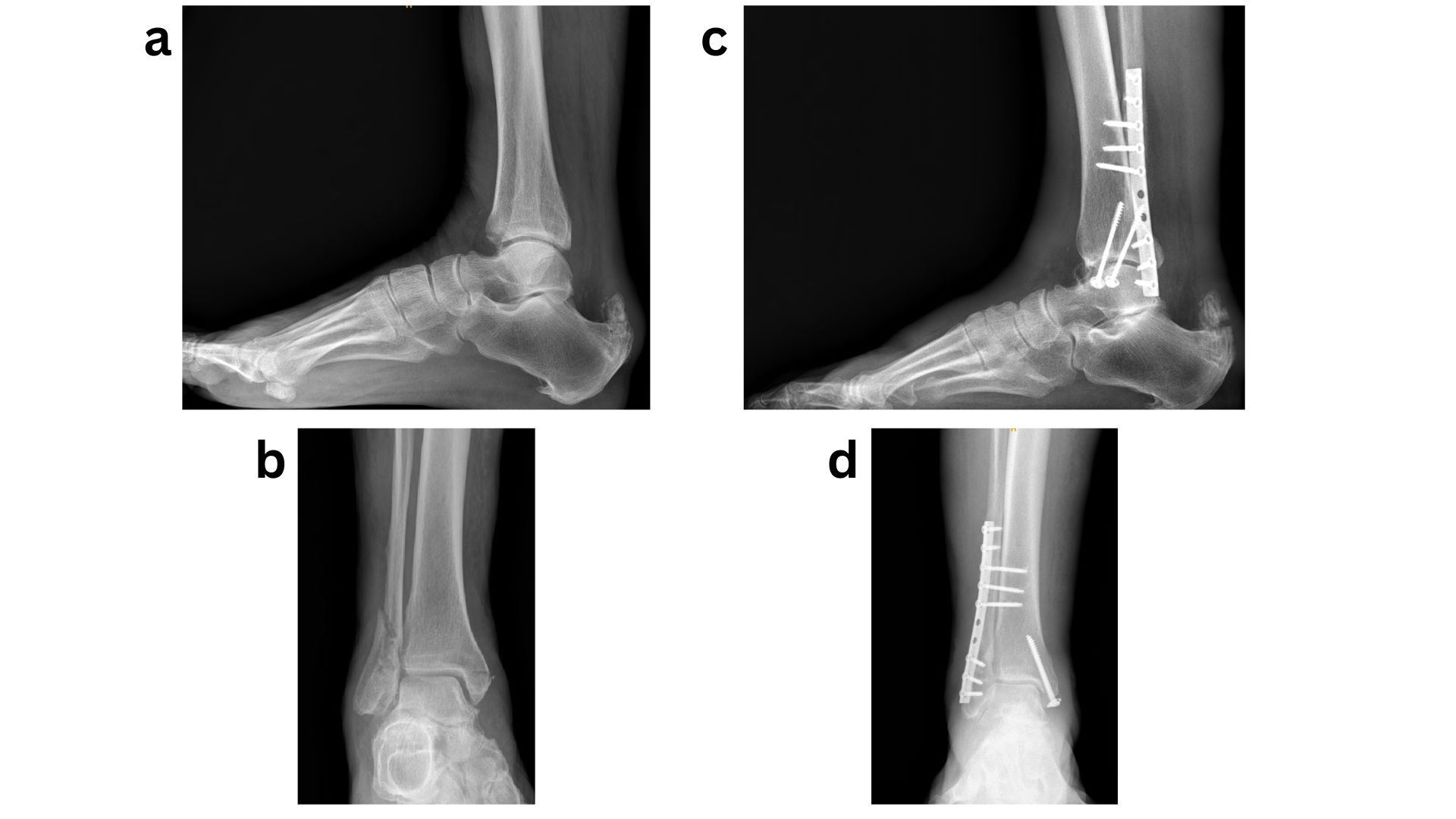
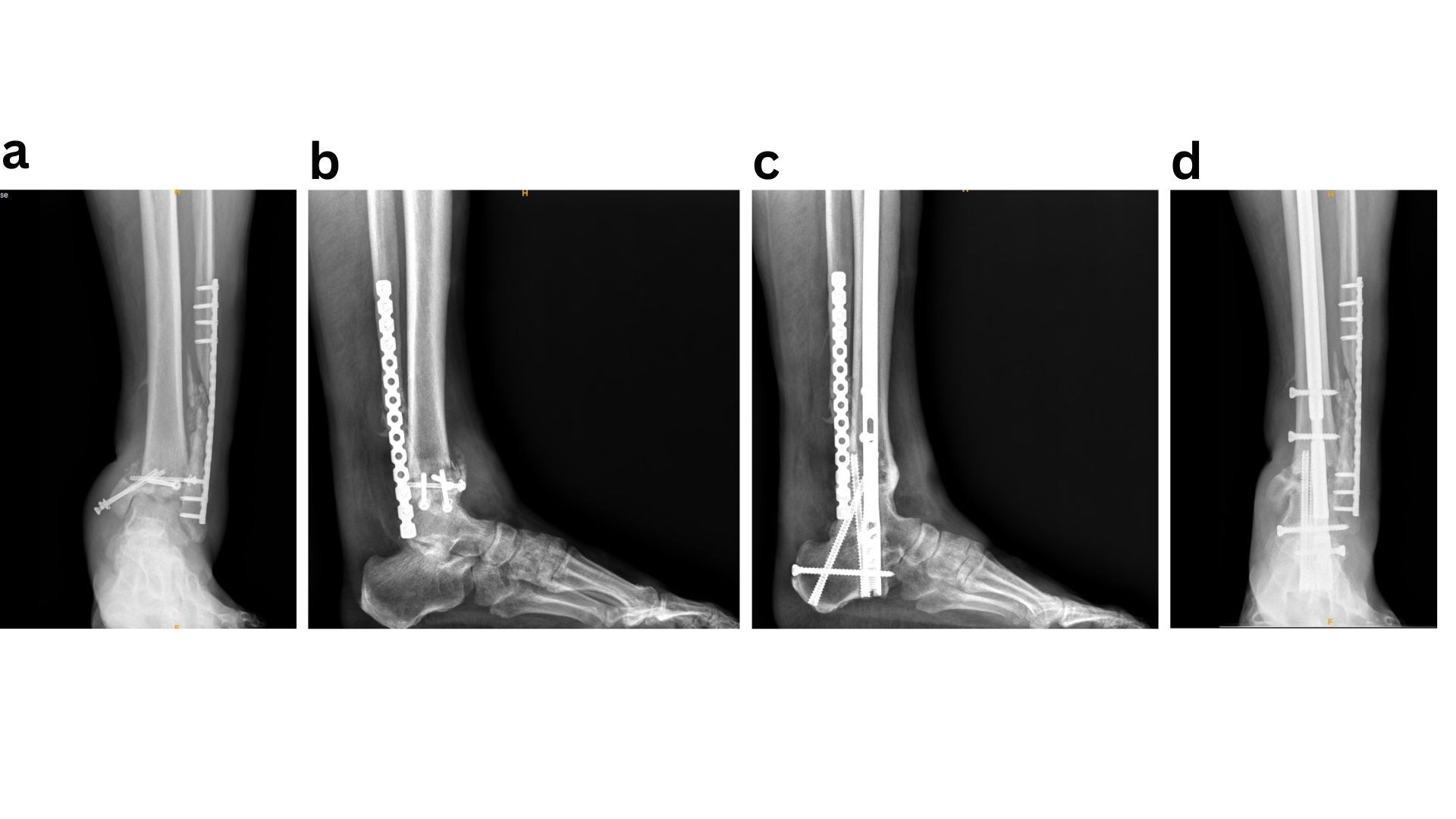
Given that the most severe complications following ORIF of diabetic ankle fractures include the development of Charcot neuroarthropathy or progression to amputation, it is logical to apply principles commonly used in Charcot reconstruction and limb salvage to this patient population. Accordingly, a “modified super construct” or “ORIF plus” strategy has been adopted for the fixation and management of diabetic ankle fractures. Sammarco et al. originally described the super construct concept in Midfoot Charcot surgery as fixation that extends beyond the zone of injury, incorporates bone resection to facilitate deformity correction and reduce soft-tissue tension, employs the strongest fixation tolerated by the soft-tissue envelope, and is applied to optimise mechanical stability.37 These principles should be adapted to diabetic ankle fractures by extending fixation beyond the immediate fracture zone, carefully planning incisions to allow fixation in areas with lower risk of wound complications, utilising the most robust fixation constructs available, and applying them in a mechanically advantageous manner, such as antiglide plating.38 The introduction of locking plate technology has significantly improved fixation in this setting by providing enhanced mechanical stability while preserving periosteal blood supply, which is critical for fracture healing, often without increasing implant bulk. In addition, the use of multiple tricortical/ quadricortical syndesmotic screws has been advocated. In neuropathic ankle fractures, it is routine practice to place three to four syndesmotic screws irrespective of initial evidence of syndesmotic injury, with the aim of maximising construct stability (Fig 1)39. Ankle fracture fixation using standard ORIF techniques is prone to failure when fundamental fixation principles are not rigorously followed. In such cases, limb salvage is best achieved through application of the superconstruct principle, with hindfoot arthrodesis (Fig 2).
The British Orthopaedic Foot & Ankle Society also advocates consideration of minimally invasive techniques, such as fibular nailing or cannulated screw fixation, in selected fracture patterns where soft-tissue compromise is a concern. Ashman et al. demonstrated the effectiveness of percutaneous fibular nail fixation in unstable Weber B and C fractures among diabetic patients, reporting a low rate of wound complications while maintaining adequate fracture stability.40
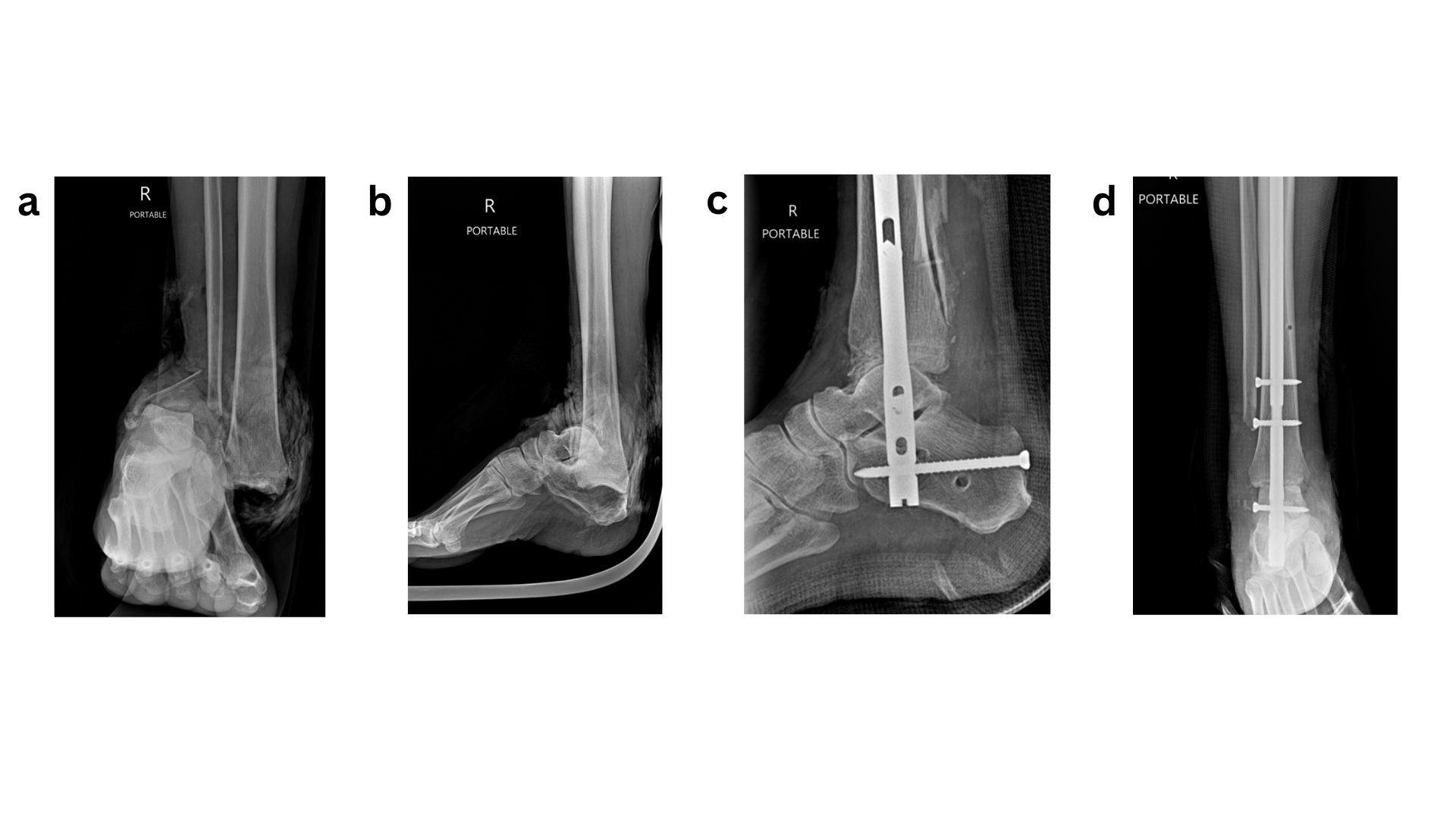
For more complex cases, particularly in the setting of complicated diabetes especially severe neuropathy, BOFAS recommends primary arthrodesis using tibio-talo-calcaneal (TTC) nailing as a limb-salvage strategy (Fig 3). Ebaugh et al. reported high limb salvage rates following primary TTC arthrodesis with retrograde hindfoot nails, with most patients maintaining ambulatory function despite a moderate complication rate. The ability to allow earlier weight-bearing with retrograde hindfoot nails, compared with prolonged immobilisation required by other fixation methods, likely contributed to favourable union rates and reduced certain complications. This approach should therefore be strongly considered in complex or limb-threatening presentations.41
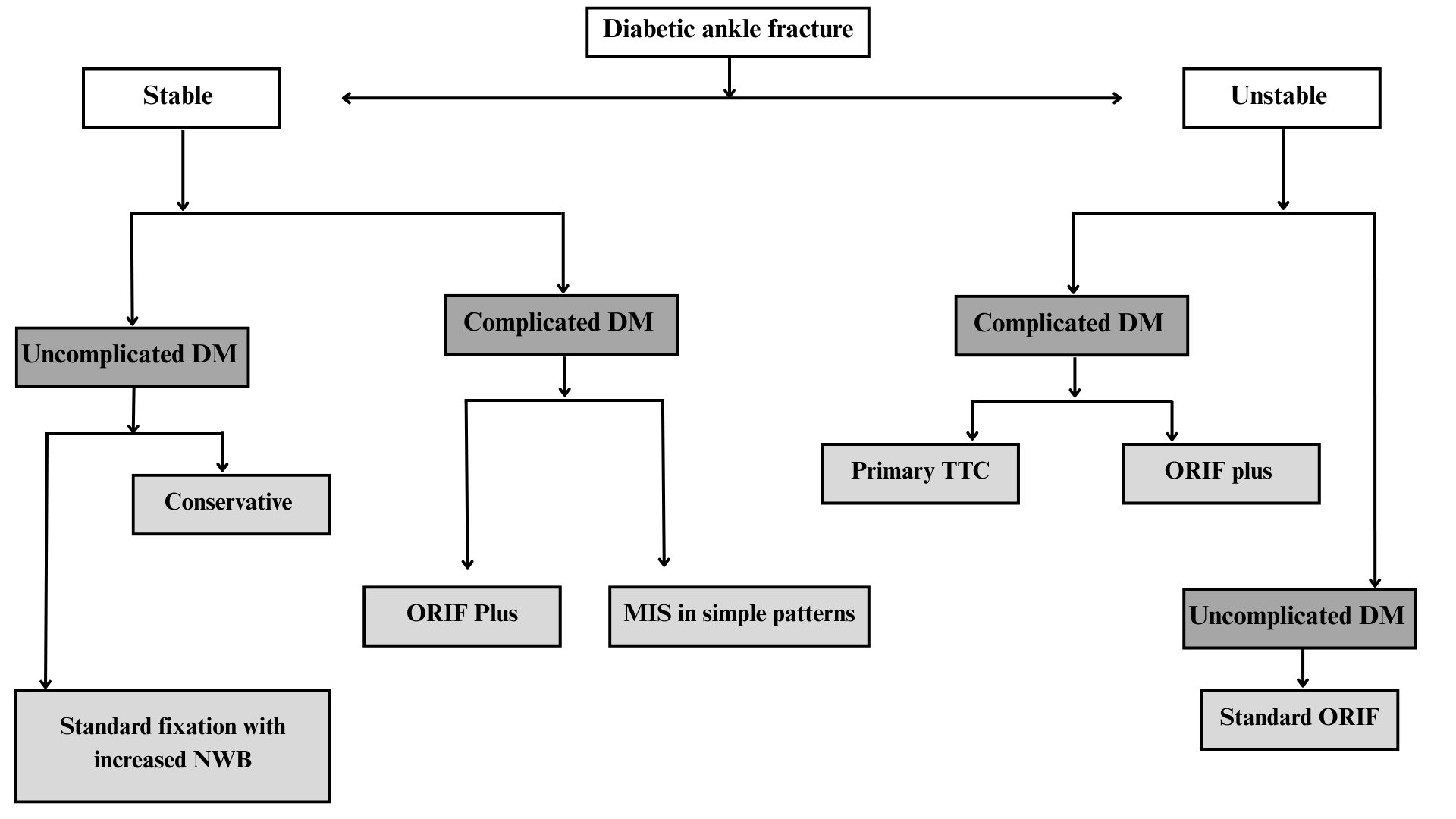
Overall, there is no uniform treatment strategy for diabetic ankle fractures. Optimal management requires an individualized approach that accounts for fracture pattern, injury severity, soft-tissue condition, and patient-specific factors, particularly the presence and extent of complicated diabetes (Fig 4).
- Complications of Ankle Fractures in Diabetes
- Infection
Surgical site infection is the most frequently reported complication following ankle fractures in patients with diabetes. Both superficial and deep infections occur at significantly higher rates compared with nondiabetic patients, particularly in those with complicated diabetes.42 Large cohort studies demonstrate that complicated diabetes markedly increases both the severity and likelihood of postoperative infection, whereas uncomplicated diabetes does not appear to confer a comparable risk.43
6.2 Impaired fracture healing
Diabetes adversely affects fracture union, with a substantially increased risk of delayed union, non-union, and malunion.44 Peripheral neuropathy, poor glycaemic control, and prolonged operative duration are consistently identified as major predictors of impaired bone healing, reflecting the detrimental effects of hyperglycaemia and neuropathy on bone metabolism and repair mechanisms.45
6.3Amputation
Although relatively uncommon, amputation represents the most severe complication following ankle fracture surgery in diabetic patients. The risk is significantly higher than in nondiabetic populations and is further amplified in open fractures, which are considered limb-threatening due to high rates of infection and wound complications.46 Population-based studies consistently report increased rates of reoperation, readmission, mortality, and amputation, particularly among insulin-dependent patients.14
6.4 Charcot neuroarthropathy
Although patients with neuropathy who sustain ankle fractures are thought to be at increased risk of developing a Charcot event, further studies are required to confirm this association. Features of Charcot arthropathy may be present at initial presentation, and surgeons should maintain a high index of suspicion, particularly in the presence of neuropathy, atypical comminution, unusual fracture patterns, or poor bone quality. Early recognition is critical, as timely identification of Charcot changes has been shown to play a key role in preventing progression to severe foot and ankle deformity.47
- Clinical implications
These findings underscore that diabetes is a heterogeneous condition, with complication risks varying according to disease severity, insulin dependence, and the presence of end-organ damage. Individualised treatment strategies that account for complicated diabetes and associated comorbidities are therefore essential to minimise complications, optimise outcomes, and maximise the potential for limb salvage.
- Conclusion
Clinical challenge: Diabetic ankle fractures are complicated by neuropathy, vascular disease, altered bone metabolism, and systemic comorbidities.
Healing risks: These factors increase the likelihood of delayed healing, malunion, nonunion, infection, Charcot arthropathy, amputation, and mortality.
Assessment: Comprehensive preoperative evaluation is essential for accurate risk stratification and planning.
Management approach:
- Stable fractures in uncomplicated diabetes may be treated conservatively.
- Unstable fractures usually require augmented fixation (“ORIF plus”).
- Multidisciplinary approach
Guiding principle: The “rule of two” supports stronger fixation, longer non-weightbearing, and closer follow-up.
9. References
1. Elsoe R, Ostgaard SE, Larsen P. Population-based epidemiology of 9767 ankle fractures. Foot and Ankle Surgery. 2018;24(1):34–9.
2. Court-Brown CM, Duckworth AD, Clement ND, McQueen MM. Fractures in older adults. A view of the future? Injury. 2018;49(12):2161–6.
3. Kannus P, Palvanen M, Niemi S, Parkkari J, Jrvinen M. Increasing number and incidence of low-trauma ankle fractures in elderly people: finnish statistics during 1970–2000 and projections for the future. Bone. 2002;31(3):430–3.
4. Regan DK, Manoli A, Hutzler L, Konda SR, Egol KA. Impact of Diabetes Mellitus on Surgical Quality Measures After Ankle Fracture Surgery. J Orthop Trauma. 2015;29(12):e483–6.
5. Wong E, Backholer K, Gearon E, Harding J, Freak-Poli R, Stevenson C, et al. Diabetes and risk of physical disability in adults: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2013;1(2):106–14.
6. Maiti S, Akhtar S, Upadhyay AK, Mohanty SK. Socioeconomic inequality in awareness, treatment and control of diabetes among adults in India: Evidence from National Family Health Survey of India (NFHS), 2019–2021. Sci Rep. 2023;13(1):2971.
7. Jiao H, Xiao E, Graves DT. Diabetes and Its Effect on Bone and Fracture Healing. Curr Osteoporos Rep. 2015;13(5):327–35.
8. Manchanda K, Nakonezny P, Sathy AK, Sanders DT, Starr AJ, Wukich DK. A systematic review of ankle fracture treatment modalities in diabetic patients. J Clin Orthop Trauma. 2021;16:7–15.
9. Lanzetti RM, Lupariello D, Venditto T, Guzzini M, Ponzo A, De Carli A, et al. The role of diabetes mellitus and BMI in the surgical treatment of ankle fractures. Diabetes Metab Res Rev. 2018;34(2):e2954.
10. Lopez-Capdevila L, Rios-Ruh JM, Fortuño J, Costa AE, Santamaria-Fumas A, Dominguez-Sevilla A, et al. Diabetic ankle fracture complications: a meta-analysis. Foot and Ankle Surgery. 2021;27(7):832–7.
11. Lovy AJ, Dowdell J, Keswani A, Koehler S, Kim J, Weinfeld S, et al. Nonoperative Versus Operative Treatment of Displaced Ankle Fractures in Diabetics. Foot Ankle Int. 2017;38(3):255–60.
12. Connolly JF, Csencsitz TA. Limb Threatening Neuropathic Complications From Ankle Fractures in Patients With Diabetes. Clin Orthop Relat Res. 1998;348:212–9.
13. Gehling DJ, Lecka-Czernik B, Ebraheim NA. Orthopedic complications in diabetes. Bone. 2016;82:79–92.
14. Liu JW, Ahn J, Raspovic KM, Liu GT, Nakonezny PA, Lavery LA, et al. Increased Rates of Readmission, Reoperation, and Mortality Following Open Reduction and Internal Fixation of Ankle Fractures Are Associated With Diabetes Mellitus. The Journal of Foot and Ankle Surgery. 2019;58(3):470–4.
15. Pincus D, Veljkovic A, Zochowski T, Mahomed N, Ogilivie-Harris D, Wasserstein D. Rate of and Risk Factors for Intermediate-Term Reoperation After Ankle Fracture Fixation: A Population-Based Cohort Study. J Orthop Trauma. 2017;31(10):e315–20.
16. Catalfamo D, Britten T, Storch D, Calderon N, Sorenson H, Wallet S. Hyperglycemia induced and intrinsic alterations in type 2 diabetes‐derived osteoclast function. Oral Dis. 2013;19(3):303–12.
17. Botolin S, McCabe LR. Chronic hyperglycemia modulates osteoblast gene expression through osmotic and non‐osmotic pathways. J Cell Biochem. 2006;99(2):411–24.
18. Tanios M, Brickman B, Cage E, Abbas K, Smith C, Atallah M, et al. Diabetes and Impaired Fracture Healing: A Narrative Review of Recent Literature. Curr Osteoporos Rep. 2022;20(5):229–39.
19. Akune T, Ogata N, Hoshi K, Kubota N, Terauchi Y, Tobe K, et al. Insulin receptor substrate-2 maintains predominance of anabolic function over catabolic function of osteoblasts. J Cell Biol. 2002;159(1):147–56.
20. Bahney CS, Hu DP, Miclau T, Marcucio RS. The Multifaceted Role of the Vasculature in Endochondral Fracture Repair. Front Endocrinol (Lausanne). 2015;6:4.
21. Jani MM, Ricci WM, Borrelli J, Barrett SE, Johnson JE. A Protocol for Treatment of Unstable Ankle Fractures Using Transarticular Fixation in Patients with Diabetes Mellitus and Loss of Protective Sensibility. Foot Ankle Int. 2003;24(11):838–44.
22. Johnson MJ, Kandasamy S, Raspovic KM, Manchanda K, Liu GT, VanPelt MD, et al. Fractures and dislocations of the foot and ankle in people with diabetes: a literature review. Ther Adv Endocrinol Metab. 2023;14.
23. Gougoulias N, Oshba H, Dimitroulias A, Sakellariou A, Wee A. Ankle fractures in diabetic patients. EFORT Open Rev. 2020;5(8):457–63.
24. Herscovici D, Scaduto JM, Early JS, Pinzur MS, Sammarco VJ. Management of Acute Ankle Fractures in Patients With Diabetes. Instr Course Lect. 2024;73:197–207.
25. Phyo N, Wee A. Managing Acute Ankle and Hindfoot Fracture in Diabetic Patients. Foot Ankle Clin. 2022;27(3):639–54.
26. Chaudhary SB, Liporace FA, Gandhi A, Donley BG, Pinzur MS, Lin SS. Complications of Ankle Fracture in Patients With Diabetes. Journal of the American Academy of Orthopaedic Surgeons. 2008;16(3):159–70.
27. McCormack RG, Leith JM. Ankle fractures in diabetics: Complications of surgical management. J Bone Joint Surg. 1998;80(4):689–92.
28. Flynn JM, Rio FR del, Pizá PA. Closed Ankle Fractures in the Diabetic Patient. Foot Ankle Int. 2000;21(4):311–9.
29. British Orthopaedic Foot & Ankle Society (BOFAS). BOFAS Hyperbook – Diabetic Ankle Fractures [Internet]. British Orthopaedic Foot & Ankle Society. [cited 2025 Dec 20]. Available from: https://www.bofas.org.uk/hyperbook/trauma/ankle-fracture/diabetic-ankle-fractures
30. Wukich DK, Joseph A, Ryan M, Ramirez C, Irrgang JJ. Outcomes of Ankle Fractures in Patients with Uncomplicated versus Complicated Diabetes. Foot Ankle Int. 2011;32(2):120–30.
31. Schon LC, Marks RM. The management of neuroarthropathic fracture-dislocations in the diabetic patient. Orthop Clin North Am. 1995;26(2):375–92.
32. Wukich DK, Kline AJ. The Management of Ankle Fractures in Patients with Diabetes. The Journal of Bone and Joint Surgery-American Volume. 2008;90(7):1570–8.
33. Jones KB, Maiers-Yelden KA, Marsh JL, Zimmerman MB, Estin M, Saltzman CL. Ankle fractures in patients with diabetes mellitus. J Bone Joint Surg Br. 2005;87-B(4):489–95.
34. Costigan W, Thordarson DB, Debnath UK. Operative Management of Ankle Fractures in Patients with Diabetes Mellitus. Foot Ankle Int. 2007;28(1):32–7.
35. Bazarov I, Peace RA, Lagaay PM, Patel SB, Lyon LL, Schuberth JM. Early Protected Weightbearing After Ankle Fractures in Patients With Diabetes Mellitus. The Journal of Foot and Ankle Surgery. 2017;56(1):30–3.
36. Chiodo CP, Macaulay AA, Palms DA, Smith JT, Bluman EM. Patient Compliance with Postoperative Lower-Extremity Non-Weight-Bearing Restrictions. Journal of Bone and Joint Surgery. 2016;98(18):1563–7.
37. Sammarco VJ. Superconstructs in the Treatment of Charcot Foot Deformity: Plantar Plating, Locked Plating, and Axial Screw Fixation. Foot Ankle Clin. 2009;14(3):393–407.
38. Manway JM, Blazek CD, Burns PR. Special Considerations in the Management of Diabetic Ankle Fractures. Curr Rev Musculoskelet Med. 2018;11(3):445–55.
39. Perry MD, Taranow WS, Manoli A, Carr JB. Salvage of failed neuropathic ankle fractures: use of large-fragment fibular plating and multiple syndesmotic screws. J Surg Orthop Adv. 2005;14(2):85–91.
40. Ashman BD, Kong C, Wing KJ, Penner MJ, Bugler KE, White TO, et al. Fluoroscopy-guided reduction and fibular nail fixation to manage unstable ankle fractures in patients with diabetes. Bone Joint J. 2016;98-B(9):1197–201.
41. Ebaugh MP, Umbel B, Goss D, Taylor BC. Outcomes of Primary Tibiotalocalcaneal Nailing for Complicated Diabetic Ankle Fractures. Foot Ankle Int. 2019;40(12):1382–7.
42. Lillmars SA, Meister BR. Acute trauma to the diabetic foot and ankle. Current Opinion in Orthopedics. 2001;12(2):100–5.
43. Wukich DK, Lowery NJ, McMillen RL, Frykberg RG. Postoperative Infection Rates in Foot and Ankle Surgery. J Bone Joint Surg. 2010;92(2):287–95.
44. Lavery LA, Lavery DC, Green T, Hunt N, La Fontaine J, Kim PJ, et al. Increased Risk of Nonunion and Charcot Arthropathy After Ankle Fracture in People With Diabetes. The Journal of Foot and Ankle Surgery. 2020;59(4):653–6.
45. Shibuya N, Humphers JM, Fluhman BL, Jupiter DC. Factors Associated with Nonunion, Delayed Union, and Malunion in Foot and Ankle Surgery in Diabetic Patients. The Journal of Foot and Ankle Surgery. 2013;52(2):207–11.
46. White CB, Turner NS, Lee GC, Haidukewych GJ. Open Ankle Fractures in Patients With Diabetes Mellitus. Clin Orthop Relat Res. 2003;414:37–44.
47. Chantelau E. The perils of procrastination: effects of early vs. delayed detection and treatment of incipient Charcot fracture. Diabetic Medicine. 2005;22(12):1707–12.