Developmental Dysplasia of the Hip: Current Concepts in Early Detection and Management
Introduction
Congenital dislocation of the hip has been known at least since antiquity, but much of the work in understanding and treating it has been in the post-Roentgenographic era. Congenital dislocation of hip is now referred to as developmental dysplasia of the hip (DDH), since it is a huge spectrum, ranging from asymptomatic mild acetabular dysplasia to frank dislocated hips1-2. The incidence of DDH varies according to time and population studied, but globally the approximated incidence is 1 to 10 per 1000 live births. Since it is a spectrum of conditions with long lasting effects, early diagnosis and appropriate treatment is of utmost importance for a healthy childhood. Early treatment can possibly prevent invasive procedures and assuring a healthy, concentric hip joint for the future. Many nations have neonatal hip screening programs; these can help in early detection and early treatment3. Developing nations where institutional births are not a norm, still see many dysplastic hips being missed and presenting late in the walking age group.
Natural History
Hip instability as assessed by Barlow and Ortolani tests are common in the first few months of life, more so in girls. Spontaneous improvement is seen in up to 90% infants who had initial instability4. This occurs because of gradual decrease in the maternal relaxin hormone in the infant blood and the improvement in the muscle tone. Persistent untreated dysplastic hip leads to altered hip biomechanics owing to decreased joint congruency. The link between early hip arthritis and untreated dysplasia of acetabulum is well established5-6. Unilateral dislocated hips when untreated, will develop limb length discrepancy, gait abnormalities, genu valgum and other sequelae. Bilateral dislocated hips may present with waddling gait, exaggeration of the lordosis and back pain.
Clinical features
The diagnosis of DDH in early infancy is mainly clinical. The two classic maneuvers widely used are: Barlow test, which assesses if a hip can be dislocated and the Ortolani test, which assesses if the dislocated hip can be reduced7. Barlow test is done in supine position with hips at 90˚ flexion and posterior axial pressure to dislocate the hip, Ortolani test involves gentle abduction and anterior lifting of femur, to reduce the dislocated hip joint.
Other important clinical features include reduced hip abduction, asymmetrical thigh and gluteal folds. There would be apparent limb discrepancy, in case of dislocated hips (Galeazzi sign).
When there is a delay in diagnosis or a neglect and the child presents after infancy in the walking age-group. There will be a Trendelenburg gait, because the dislocated and high riding femoral head will cause abductor weakness. The limb length discrepancy will be more marked. Children with bilateral dislocation may present with excessive lumbar lordosis due to hip flexion contractures and symmetrical restricted hip abduction.
Imaging
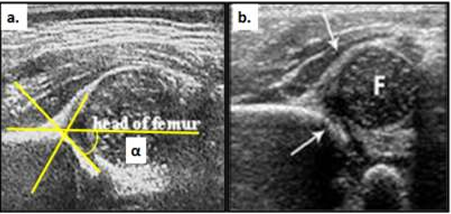
Ultrasonography (USG) of hip is the most commonly employed diagnostic method in early infancy since most of the acetabulum and femoral head is cartilaginous. Although there are various methods of quantifying the acetabular dysplasia, most commonly used is the one described by Graf8. The timing of USG screening has been debated based on whether a universal or a selective USG screening protocol is followed, however delaying USG screening by 4-6 weeks seems most pertinent, since most of the hip instability at birth resolves by 4 weeks9. The Graf method employes measurement of two angles: alpha angle or acetabular roof angle which is measured between the ilium and osseous acetabular wall, elaborated in Fig 1, should be > 60˚, and the beta angle, between ilium and the labral cartilage, which should be < 50˚. Dynamic USG (Harcke’s method) can assess stability of the hip under stress maneuvers. USG is also used to evaluate the effectiveness of harness treatment.
Since, universal USG screening carries high risk of high false positives, American Academy of Paediatrics (AAP) recommends selective screening for infants with high risk10. Risk factors predisposing to dysplasia of hip are: positive family history, first born, girl child, multiple gestation, breech presentation, oligohydramnios11.
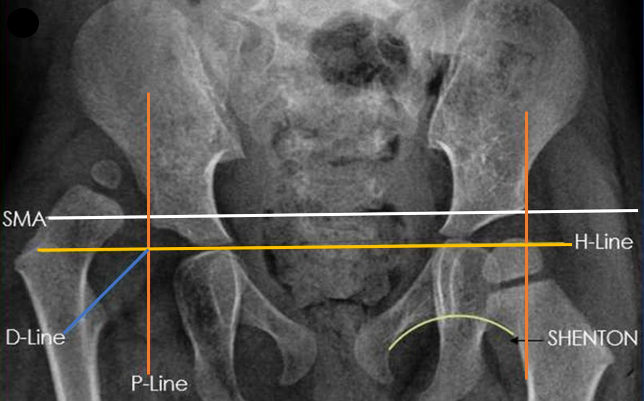
Plain radiographs are rarely used in the neonatal period or for routine early screening since the cartilaginous acetabulum and unossified femoral head will not be appreciated on the X-rays. However, it the stand imaging method used after 6 months. Commonly, done views are the antero-posterior (AP) view of pelvis with both hips (both patellae facing forwards), frog leg lateral view and rarely the Von Rosen view. The radiographic lines are described in Fig 2.
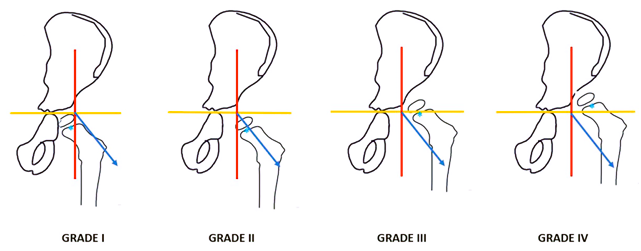
Two important classification systems are based on the antero-posterior radiograph of pelvis with both hips. The Tonnis classification takes the reference of the center of femoral head ossific nucleus and its relation to the radiographic lines to quantify the disease12. Another recent classification system is by the International Hip Dysplasia Institute (IHDI) which takes the center of the proximal femoral metaphysis (H-point) as the reference point13-14. Hence, this classification can be used even before the ossific nucleus is visible on the radiographs, the classification is explained in Fig 3.
Management
The aim of treatment of DDH is to obtain and maintain a concentric reduction of the femoral head inside the acetabulum. This will allow normal development of the hip joint as the normal forces act across the hip once the child walks. For infants younger than 6 months, bracing remains the standard of care15. Braces can broadly be categorized as dynamic – allowing some active hip movements or static braces which are rigid and don’t allow active movements. Pavlik Harness is the commonly used one for infants less than 6 months. It has shown a success rate of > 90 %16. Failure rates are higher with greater risk of AVN when the treatment is initiated after 4-6 months, the ideal time for treatment is before 6 weeks17. The duration of bracing is typically around 6-8 weeks with periodic USG monitoring to see the improvement in USG parameters.
If the USG parameters on bracing don’t show an improvement or if there is persistent subluxation or instability beyond 6 months then attempt of close reduction, confirmation of concentric reduction with arthrography, followed by hip spica casting should be done. Percutaneous adductor tenotomy facilitates the close reduction. Post reduction spica immobilization is usually with hips flexed at 90 degrees with controlled abduction. Medial open reduction is usually enough is infants in case close reduction fails.
Children above 12 months may need antero-lateral open reduction along with either femoral osteotomy or acetabular osteotomy or both. In high riding dislocations, femoral shortening will facilitate reduction of the femoral head, derotation can help in re-orienting the femoral head in cases with dysplastic acetabulum18. Usually in children less than 18 months, a concentric reduction with open reduction without a pelvic osteotomy is enough due to the remodeling potential. The role of initial concomitant pelvic osteotomy for children in the 18 months – 4 years age group requiring is debated, many surgeons opting to address the acetabular dysplasia during the open reduction. In older children or those with persistent dysplasia after initial reduction of the hip will require pelvic osteotomy since the remodeling potential is limited19. However, in children above 4 years most surgeon routinely perform pelvic osteotomy since the remodeling potential is unpredictable after that age. An overview of treatment according to age is given in Table 1.
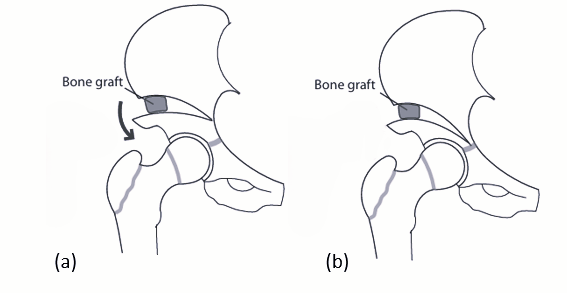
The role of pelvic osteotomy is to resolve the acetabular dysplasia and improve femoral head coverage. Various pelvic osteotomies have been described in the literature. The choice of pelvic osteotomy depends on the age of the patient, type of dysplasia, shape of acetabulum and the status of triradiate cartilage19-20. These can be broadly be classified as re-shaping osteotomies or re-directional osteotomies. Reshaping osteotomies are incomplete innominate osteotomies which are inherently stable like Dega osteotomy, Pemberton pericapsular osteotomy (among the most popular), Fig 4. Re-directional osteotomies, Fig 5 are complete osteotomies which alter acetabular orientation without changing the size or shape of the acetabulum like Salter innominate osteotomy, triple pelvic osteotomy and Bernese periacetabular osteotomy.
Conclusion
A thorough clinical examination is of utmost importance in early diagnosis of DDH. Use of USG either as universal or selective screening has reduced the incidence of late presenting DDH. Since, the costs of surgical intervention is much greater than that of conservative management with bracing, hence, early referral and selective USG screening of high-risk children is essential, especially in developing countries21. Post treatment radiological follow-up is essential to pick up persistent acetabular dysplasia and avascular necrosis of femoral head. The choice of pelvic osteotomies is influenced by multiple factors and should be treated promptly to reduce risk of early degenerative changes in the hip.
References
- Klisic PJ: Congenital dislocation of the hip--a misleading term: brief report. J Bone Joint Surg Br. 1989.
- Aronsson DD, Goldberg MJ, Kling TF Jr, Roy DR: Developmental dysplasia of the hip. Pediatrics. 1994, 94:201-8.
- Shorter D, Hong T, Osborn DA. Cochrane Review: Screening programmes for developmental dysplasia of the hip in newborn infants. Evid Based Child Health. 2013 Jan;8(1):11-54.
- Vaquero-Picado A, González-Morán G, Garay EG, Moraleda L: Developmental dysplasia of the hip: update of management. EFORT Open Rev. 2019, 4:548-56.
- Engesaeter LB, Furnes O, Havelin LI: Developmental dysplasia of the hip--good results of later total hip arthroplasty: 7135 primary total hip arthroplasties after developmental dysplasia of the hip compared with 59774 total hip arthroplasties in idiopathic coxarthrosis followed for 0 to 15 years in the Norwegian Arthroplasty Register. J Arthroplasty. 2008, 23:235-40.
- Wedge JH, Wasylenko MJ: The natural history of congenital disease of the hip. J Bone Joint Surg Br. 1979, 61-B:334-8.
- Sulaiman AR, Yusof Z, Munajat I, Lee NAA, Nik Z. Developmental Dysplasia of Hip Screening Using Ortolani and Barlow Testing on Breech Delivered Neonates. Malays Orthop J. 2011;5(3):13-16.
- Graf, R. (1980). The diagnosis of congenital hip-joint dislocation by the ultrasonic Combound treatment. Archives of Orthopaedic and Trauma Surgery, 97, 117–133.
- Boeree, N. R., & Clarke, N. M. (1994). Ultrasound imaging and secondary screening for congenital dislocation of the hip. The Journal of Bone and Joint Surgery, 76B, 525–533.
- Hauk, L. (2017). Developmental dysplasia of the hip in infants: A clinical report from the AAP on evaluation and referral. American Family Physician, 96(3), 196–197.
- Agarwal, A., & Guppta, N. (2012). Risk factors and diagnosis of developmental dysplasia of hip in children. Journal of Clinical Orthopaedics and Trauma, 3(1), 10–14.
- Tönnis, D. (1985). Indications and time planning for operative interventions in hip dysplasia in child and adulthood. Zeitschrift fur Orthopadie und Ihre Grenzgebiete, 123, 458–461.
- Narayanan, U., Mulpuri, K., Sankar, W. N., et al. (2015). Reliability of a new radiographic classification for developmental dysplasia of the hip. Journal of Pediatric Orthopedics, 35, 478–484.
- Karnik, A., Lawande, A., Lawande, M. A., Patkar, D., Aroojis, A., & Bhatnagar, N. (2021). Practice essentials of imaging in early diagnosis of DDH. JOIO.
- Merchant, R., Singh, A., Dala-Ali, B., Sanghrajka, A. P., & East wood, D. M. (2021). Principles of bracing in the early management of developmental dysplasia of the hip. JOIO.
- Cashman, J. P., Round, J., Taylor, G., & Clarke, N. M. P. (2002). The natural history of developmental dysplasia of the hip after early supervised treatment in the Pavlik harness. A prospective, longitudinal follow-up. The Journal of Bone and Joint Surgery. British volume., 84(3), 418–425.
- Agostiniani R, Atti G, Bonforte S, Casini C, Cirillo M, De Pelegrin M, et al. Recommendations for early diagnosis of Developmental Dysplasia of the Hip (DDH): working group intersociety consensus document. Ital J Pediatr [Internet]. 2020 Oct 9;46(1):150.
- Gholve PA, Flynn JM, Garner MR, Millis MB, Kim YJ: Predictors for secondary procedures in walking DDH. J Pediatr Orthop. 2012, 32:282-9.
- Venkatadass K, Durga Prasad V, Al Ahmadi NMM, Rajasekaran S. Pelvic osteotomies in hip dysplasia: why, when and how? EFFORT Open Rev. 2022 Feb 15;7 (2):153-163.
- Wang CW, Wu KW, Wang TM, Huang SC & Kuo KN. Comparison of acetabular anterior coverage after Salter osteotomy and Pemberton acetabuloplasty: a long-term follow up. Clinical Orthopaedics and Related Research 2014. 472 1001–1009.
- Pandey, R.A., & Johari, A. N. (2021). Screening of newborns and infants for developmental dysplasia of the hip: systematic review. JOIO.
Fig 1: USG of hip, (a) shows a normal hip with the angle between central ilial line and acetabular roof, alpha angle of > 60. Angle between the central ilial line and labrum is beta angle, (b) shows a femoral head with is subluxated and a dysplastic acetabulum with reduced alpha angle.
Fig 2: Pelvis with both hips antero-posterior view showing x-ray. H-line is the Hilgenreiner's line drawn from the outer margin of the acetabulum. P-line is the Perkin's line passes through the triradiate cartilage. SMA is the superior margin of acetabulum line which joins both lateral acetabular sourcils. D-line is the diagonal line from the intersection of H and P lines at 45˚. Shenton line is drawn from the inferior neck surface to the superior margin of obturator foramen.
Fig 3: IHDI classification of DDH. Yellow line - H (Hilgenreiner) line, red line - P (Perkin) line, blue line—D (Diagonal) line, blue dots at the centre of metaphysis – H point.
Fig 4: Reshaping acetabular osteotomies, (a) Dega acetabuloplasty, (b) Pemberton acetabuloplasty
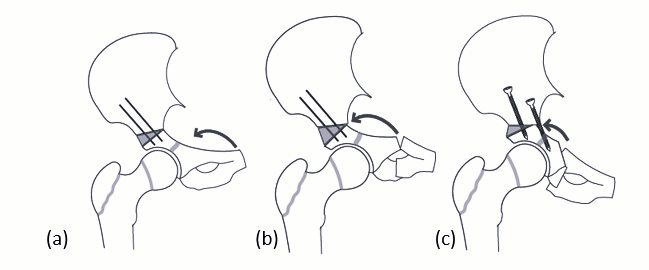
Fig 5: Redirecting osteotomies, (a) Salter innominate osteotomy, (b) triple pelvic osteotomy, (c) Periacetabular osteotomy.
Age of Child | Preferred Treatment |
|---|---|
Up to 6 months | Pavlik Harness |
6 – 12 months | Close Reduction or Medial open reduction |
12-24 months | Close Reduction or anterolateral open reduction |
2 years – 8 years | Anterolateral open reduction of hip +/- femoral osteotomy +/- pelvic osteotomy |
Table 1: Preferred treatment according to age.