MASSIVE HETEROTOPIC OSSIFICATION EXCISION AND TOTAL HIP ARTHROPLASTY IN A BELOW KNEE AMPUTEE WITH MALUNITED ACETABULUM AND PROTRUSIO: A CASE REPORT
Abstract
Case:
A 28-year-old man, who had previously undergone open reduction and internal fixation (ORIF) of the right acetabulum and a below-knee amputation after a high-velocity motor vehicle accident, presented with a stiff hip and inability to independently don his prosthesis. Imaging revealed massive heterotopic ossification (HO) with both intra- and extra-articular ankylosis of the right hip. He underwent single-stage HO excision and conversion total hip arthroplasty (cTHA), with excellent clinical and radiographic outcomes at 1-year follow-up.
Conclusion:
Conversion THA in the setting of massive HO and acetabular malunion is technically demanding and requires meticulous preoperative planning. Advances such as three-dimensional (3D) modelling can aid in safe HO excision, neurovascular protection, and precise implant positioning, ultimately leading to excellent functional recovery.
Keywords: Heterotopic Ossification, Ankylosis, Total hip arthroplasty, 3D print
Introduction
Conversion total hip arthroplasty (cTHA) following acetabular fracture fixation is among the most challenging reconstructive procedures in orthopaedics1. The presence of heterotopic ossification (HO) further complicates exposure and component placement. HO is a recognized complication after acetabular surgery2, with severity commonly described using the Brooker classification, which also correlates with function and outcomes3.
Excision of HO is the treatment of choice for extra-articular ankylosis, but preoperative planning is difficult, particularly in massive mature HO associated with intra-articular ankylosis. Computed tomography (CT) is the gold standard for mapping HO, and the use of 3D-printed pelvic models offers a valuable tool to simulate safe dissection planes and plan reconstruction4.
We present a rare case of combined intra- and extra-articular hip ankylosis due to massive HO in a young man with acetabular malunion and ipsilateral below-knee amputation, managed successfully with single-stage HO excision and cTHA using 3D-printed model–based planning.
Case :
A 28-year-old man presented with chronic low back pain and inability to bend for prosthesis application. Three years earlier, he sustained a high-energy motor vehicle accident resulting in a right acetabular fracture and ipsilateral lower limb crush injury. He was treated elsewhere with staged ORIF of the pelvis and acetabulum and a right below-knee amputation.
On examination his right hip had a well-healed scar and was fused in 5° flexion and 15° abduction with no movement in any plane. Laboratory markers (ESR – 28 mm/hr, CRP – 4 mg/L, ALP – 65 U/L) were normal .
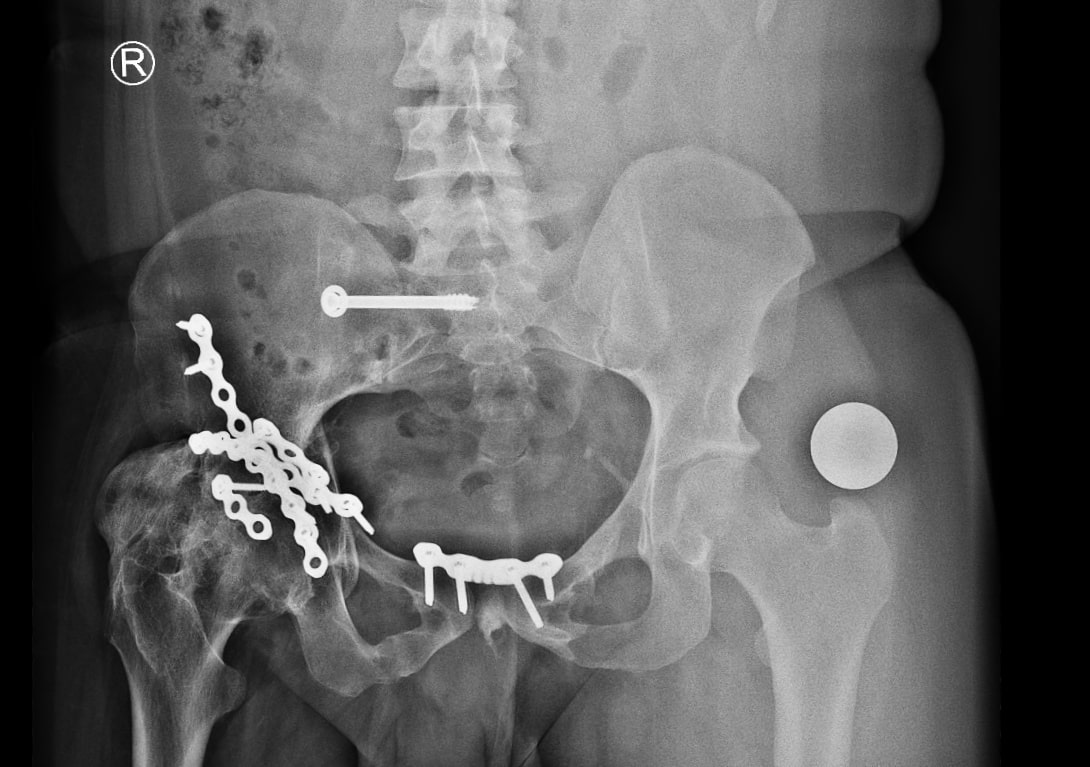
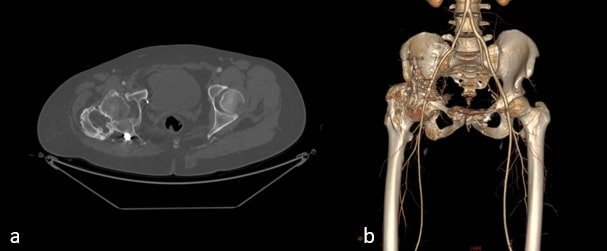
Radiographs demonstrated malunited anterior and posterior columns with retained implants, medial acetabular migration, and massive mature HO bridging the acetabulum and proximal femur (Brooker grade IV)(Fig 1). CT scan showed mal united fracture of both columns, heterotopic mass extending superior, anterior and posterior to the right proximal femur causing extra articular ankylosis(Fig 2 a). There also was intra articular ankylosis with trabeculae crossing the hip joint posteriorly fusing with the acetabulum. There was severe protrusio with intact medial wall. CT angiography superimposed images revealed the external iliac vessels closely abutting but not encased by the HO(Fig 2 b).
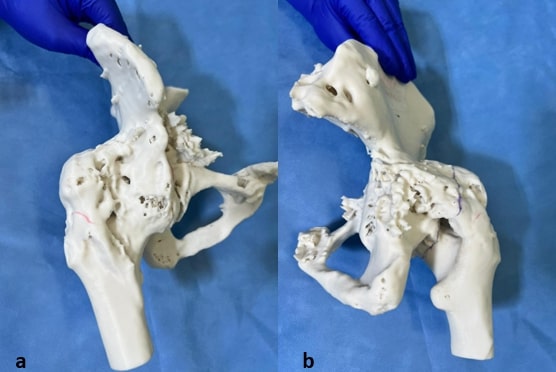
Given his age, we initially considered salvage of the joint. But with severe intra-articular fusion and acetabular deformity, joint salvage was not possible. Hence, we were left with HO excision along with hip arthroplasty. We debated whether to do this in 2 stage with HO excision initially and total hip arthroplasty at a later stage. 3D printed model of the pelvis was obtained in view of complexity of the case(Fig 3). With 3D print in hand , we felt that we could do both these procedures together with an osteotomy through the ossific mass along with neck of femur. Our next worry was how to protect the neurovascular bundle which was in close proximity to neck and HO mass anteriorly. 3D printing was helpful here, as we felt we could run a finger down the anterior neck.
Operative Technique
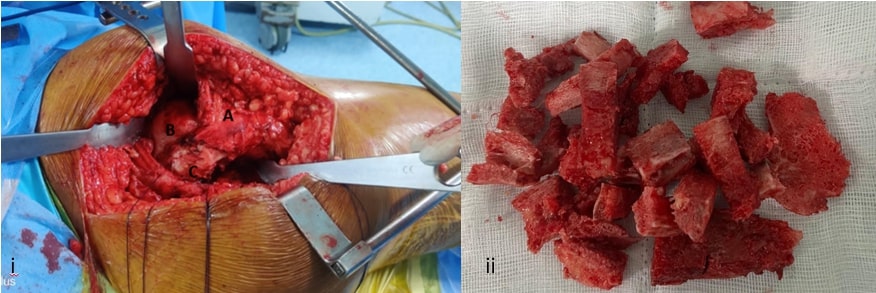
We approached the hip posteriorly with gluteus max release. Deeper dissection revealed gluteus minimus that was completely osssified. The gluteus medius was identified which was thinned out and was retracted anteriorly(Fig 4 i) . Short external rotators were tagged and incised. Capsulotomy was performed.
As planned with 3D printing, we placed three K-wires on the tip of greater trochanter and the level of osteotomy marked and proceeded. We could book open the entire HO mass and femur anteriorly. With a finger running down the anterior part of HO protecting the neurovascular bundle , careful piecemeal resection of HO was performed. The highly vascular HO was kept aside and used as graft for subsequent medial wall reconstruction of acetabulum(Fig 4 ii). Distal femoral traction pin with 5 mm Steinman pin was used to lever the limb for manipulation because of short below knee stump. Reaming into the femoral head was done gradually till foveal fat was identified. A screw tip was seen protruding on the acetabular floor which was left as such and covered with graft. We used the excised bone to build up the protrusio by reverse reaming. Sequential reaming was done to size 54. Femur canal was then prepared and sized. An uncemented total hip arthroplasty was performed with size 54 Gription multihole cup fixed with 2 screws , 36 mm XLPE insert, Ceramic 36 mm femoral head and size 2 Accolade 2 stem. Combined anteversion of 40 degrees was achieved and the hip was found to be stable . Meticulous excision of contused muscle and proper soft tissue handling was ensured throughout the surgery. Capsule and short external rotators were repaired. Drain was placed and fascia lata was repaired. Wound was closed in layers.
Postoperative Course
Radiographs demonstrated satisfactory medial wall reconstruction, restored offset, and removal of impinging HO(Fig 5). The patient commenced weight-bearing on postoperative day 1. HO prophylaxis with indomethacin 25 mg thrice daily was prescribed for 6 weeks.
At 6 weeks, he was independently mobile and able to don his prosthesis unaided(Fig 6). At 1 year, he remained pain-free, returned to motorcycling, and radiographs revealed minimal (Brooker grade1) recurrence of HO.
Discussion
This case highlights the unique challenges of conversion THA in the setting of massive HO, intra- and extra-articular ankylosis, and ipsilateral below-knee amputation. Traditional strategies often recommend staged excision and arthroplasty. However, by employing 3D modelling technology, it was possible to clearly define the anatomical relationships between heterotopic bone and vital neurovascular structures, as well as to identify interfering implants encased within the ossified mass. The model also provided critical guidance in mapping osteotomy and excision planes, which helped to minimize blood loss and avoid unnecessary soft-tissue trauma. Previous studies emphasize CT as the gold standard for HO mapping, but reports of 3D printing–assisted planning in this scenario remain scarce. Our case demonstrates that 3D simulation can reduce operative risk and optimize functional outcomes.
Conclusion
Single-stage HO excision and conversion THA, can be a safe and effective solution in young patients with complex post-traumatic ankylosis. Preoperative 3D modelling5 allows precise planning, protects vital structures, and ensures successful functional recovery.
References:
1.Wilson JM, Abdel MP, Trousdale RT, Lewallen DG, Berry DJ. Total Hip Arthroplasty Following Operative Fixation of Acetabular Fracture: A Contemporary Series. The Journal of Arthroplasty. 2024 May;39(5):1273–8.
2.Firoozabadi R, Alton T, Sagi HC. Heterotopic Ossification in Acetabular Fracture Surgery. Journal of the American Academy of Orthopaedic Surgeons. 2017 Feb;25(2):117–24.
3.BROOKER AF, BOWERMAN JW, ROBINSON RA, RILEY LH. Ectopic Ossification Following Total Hip Replacement. The Journal of Bone & Joint Surgery [Internet]. 1973 Dec [cited 2021 Dec 2];55(8):1629–32. Available from: http://jc.dalortho.ca/wp-content/uploads/2015/02/ectopic-ossification-follow-total-hip-replacement.pdf
4.Lucas SL, Gallagher BP, Mullinix KP, Brumback RJ, Cunningham BW. 3D-Printed Model in Preoperative Planning of Sciatic Nerve Decompression Because of Heterotopic Ossification. JBJS Case Connector. 2024 Jan 1;14(1).
5.Galvez M, Asahi T, Baar A, Carcuro G, Cuchacovich N, Fuentes JA, et al. Use of Three-dimensional Printing in Orthopaedic Surgical Planning. JAAOS: Global Research and Reviews. 2018 May;2(5):e071.
ETHICAL CONSIDERATIONS:
Informed consent was obtained from the patient regarding taking his pictures and discussion of the case for academic purposes. Patient data was anonymized to protect confidentiality and our institute ethical committee clearance obtained.
AUTHORSHIP AND CONTRIBUTION:
Dr.Bipin Theruvil performed the surgery, Dr Varsha drafted the manuscript and Dr. Pooja collected the data.