Title: Comparison of functional & radiological outcomes of patients undergoing single sitting bilateral total knee replacement vs staged bilateral total knee replacement
Abstract
Background: The incidence of Osteoarthritis knee is increasing every year world over. Total knee replacement is a very established procedure done for osteoarthritis of the knee joint which is associated with deformities such as varus or valgus knee, fixed flexion deformities, hyperextension of knee. However the researches that compare both the functional and radiological outcomes in single sitting and staged total knee replacement are few.
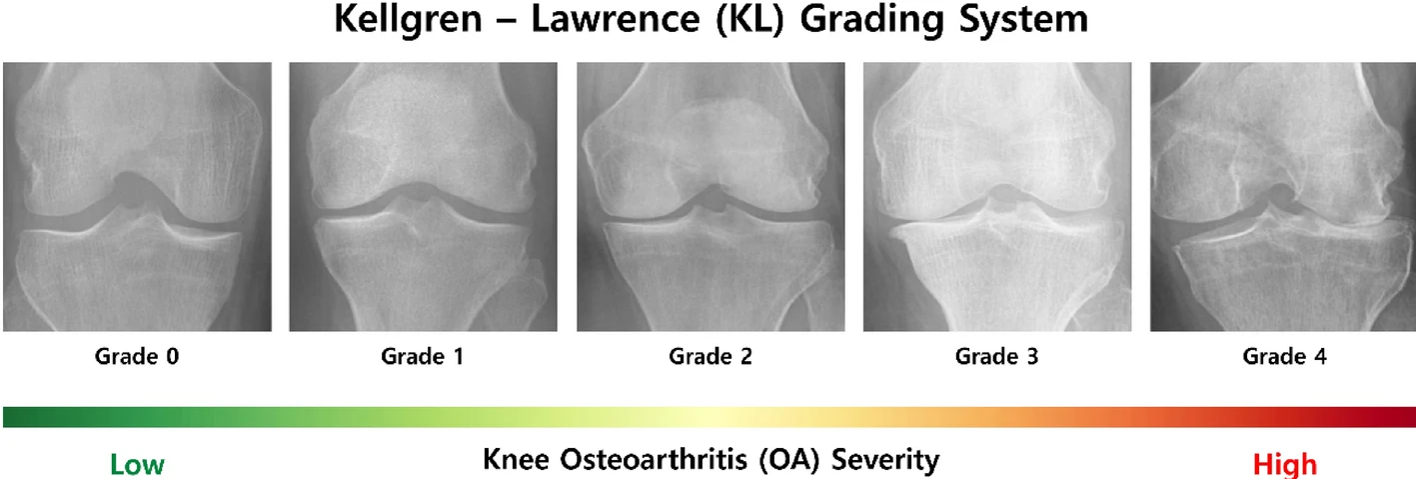
The diagnosis is confirmed by both clinical and radiological studies. Total knee replacement is done in patients with Kellgren and Lawrence stage 3 and stage 4 osteoarthritis of the knee joint. In cases of bilateral osteoarthritis knee Total knee replacement can be done as a single sitting procedure or can be done as a staged procedure.
Methods: This study compares the functional and radiological outcomes in 48 patients, i.e. 24 from each category who underwent total knee replacement under the same surgeon with similar techniques using Oxford knee score, knee society score, WOMAC score and LDFA, MPTA, coronal alignment and sagittal alignment respectively.
Results: The functional outcomes were found to be similar in both groups with better outcomes at 6 weeks in patients who underwent staged total knee replacement although the values were statistically comparable at 3 months, 6 months and 1 year (p=0.01). The radiological outcomes were also comparable between the two groups with slight deviation of radiological parameters from mean in the 2nd knee in cases of single sitting Total knee replacement.
Conclusions: Total knee replacement can be done as a single sitting or a staged procedure with no difference in functional and radiological outcome at 3 months and 6 months follow-up.
Keywords: Total knee replacement, osteoarthritis, functional outcome ,knee society score, oxford knee score
Introduction
Osteoarthritis is a musculoskeletal degenerative condition that affects weight bearing joints, predominantly the hip and knee joints and thus modifying the articular cartilage and the subchondral bone with associated changes to the Hoffa’s fat pad, synovium, muscles and ligaments [1].Sir Archibald Edward Garrod, Albert Hoffa and R. Llewellyn Jones first described osteoarthritis as a degenerative disease of the knee joint in 1890 and this was further classified by Dr. Kellgren into four different types based on the radiographic appearance of the joint (Fig 1.) [2]. The main goal of total knee replacement was restoration of knee alignment with the mechanical axis passing through the center of hip joint , knee joint and ankle joint [3]. However not just the mechanical alignment, the component alignment has also been recently considered to be important, an idea known as kinematic alignment [3].
Significant collaborations between doctors and engineers has helped in the development of improved designs of knee replacement ranging from resurfacing prosthesis to the constrained prosthesis and meniscal bearing prosthesis. Patient specific cutting guides have also been introduced recently that helps in improving the accuracy and reproducibility of bone resection and soft tissue balancing [4].
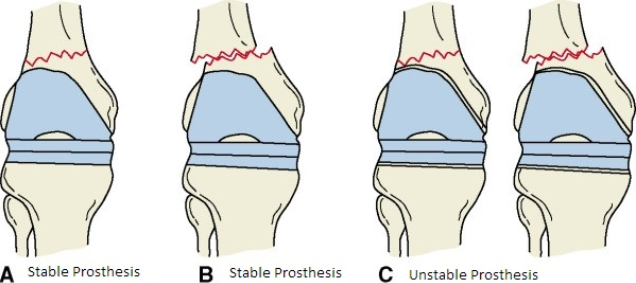
Complications that can occur following a knee replacement can include knee stiffness, periprosthetic fractures (Fig 2), prosthetic joint infection, aseptic loosing, patellar mal-tracking and heterotrophic ossification with joint infection or bacteremia being an absolute contraindication for the procedure. The designs of implants used for total knee replacement can vary from unconstrained or cruciate retaining to partially constrained implants to fully constrained implants [5].
Nowadays there is an argument going on whether the bilateral joint replacement shoulder be done as a single procedure or in a stage manner. In patients with bilateral end stage arthritis of the knee, as a single knee replacement doesn’t restore complete function, some advocate about the need for staged total knee replacement [6] There are both advantages and disadvantages for both with the disadvantages of staged procedure being separate anesthesia exposure, increased cost because of separate procedures and separate rehabilitation programs and the advantage being lesser requirement of blood transfusion and lesser incidence of fat embolism [6].
Materials and methodology
The study was approved by the institutional review board and the institutional ethics committee. Informed consent was obtained from all patients who participated in the study. All the patients who underwent total knee replacement at this hospital under the same surgeon using similar surgical techniques within the age group of 50 -80 between September of 2022 to august of 2024 were taken for the study. In cases of staged TKR, the surgery on the 2nd knee was performed with in a gap of 1 week to 1 month post the first surgery.
Patents with BMI > 35, patients with h/o any major knee surgeries and patients with osteoarthritis of the hip and ankle joints were excluded.
Cruciate retaining type of implants (fig 3) were used for all patients selected for the study and medial Parapatellar approach to knee (Fig 4) used in all cases. For closure Number 2 vicryl for the capsule and subcutaneous tissue and staples used for skin. Post-operative mobilization was started on post op day 2.
To assess the functional outcome Pre-operative Oxford knee score, knee society score and WOMAC scores were compared to the post-operative values at 6 weeks, 3 months, 6 months and 12 months. Radiological outcome was measured by comparing the pre-operative and post-operative LDFA, MPTA, coronal alignment and sagittal alignment and also comparing them to the mean values.
Results
In terms of the functional outcome, preoperatively the Oxford knee scores were 17.8 for the single sitting TKR group and 19.2 for the staged TKR group, showing no significant difference. At 6 weeks, the scores improved to 28.6 and 29.8 respectively. By 3 months, both groups had nearly identical scores of 35.3 and 35.4. However, by 6 months, a statistically significant difference emerged, with the single sitting TKR group scoring 38.7 and the staged TKR group scoring 40.2 (Table 1).
In terms of the Knee Society scores, preoperative values were 43.3 for the single sitting TKR group and 45 for the staged TKR group. At 6 weeks, scores were 69.7 and 69.2 respectively. By 3 months, both groups scored 77.2 and 77.1, showing no significant difference. At 6 months, the scores were 83.6 for the single sitting TKR group and 85.3 for the staged TKR group (Table 1).
The WOMAC scores showed a significant preoperative difference (78.8 vs. 81.3). However, at 6 weeks and 3 months, both groups had identical scores (44.4 and 33.2 respectively). By 6 months, scores were 23.7 for the single sitting TKR group and 24.2 for the staged TKR group, indicating similar outcomes (Table 1).
The improvement in the functional score was significant in the post-operative period as compared to the pre-operative values and the results were comparable between bilateral staged and single sitting groups.
On assessing the radiological outcome, in the bilateral single sitting TKR group (N=24), radiological parameters exhibited notable changes postoperatively. The lateral distal femoral angle (LDFA) increased significantly from 85.3 to 87.7. Although the medial proximal tibia angle (MPTA) improved from 85.9 to 87.5, this change was not statistically significant. Coronal alignment showed a substantial improvement, decreasing from 9.5 preoperatively to 2.0 postoperatively. Additionally, sagittal alignment improved significantly, reducing from 9.6 preoperatively to 8.1 postoperatively. These results suggest that single sitting TKR leads to significant enhancements in radiological parameters, particularly in alignment (Table 2).
The change in radiological parameters for the staged bilateral TKR group (N=24) demonstrated significant improvements postoperatively. The lateral distal femoral angle (LDFA) increased from 86.2 preoperatively to 88.2 postoperatively. The medial proximal tibia angle (MPTA) showed a slight increase from 82.9 to 83.7, which was not statistically significant. Coronal alignment improved markedly, decreasing from 9.5 preoperatively to 2.5 postoperatively. Similarly, sagittal alignment showed significant improvement, reducing from 9.3 preoperatively to 7.9 postoperatively. These findings indicate substantial postoperative radiological improvements in alignment following staged bilateral TKR (Table 3).
The change in radiological parameters assessed based on the post-operative x-rays pointed towards a good outcome in both categories of patients and the results were comparable among both groups.
Discussion
Knee pain can be due to a wide range of causes. The pain if it’s a chronic one (> 3 months) especially a bilateral knee pain, the most common etiology i.e. Osteoarthritis has to be ruled out. Most cases of osteoarthritis are bilateral and the common etiology could be obesity, secondary to inflammatory arthritis, post-traumatic arthritis. The condition can be divided into 4 stages based on x-ray findings. Stages 3 & 4 are indicative of total knee replacements unless there are absolute medical or surgical contraindications.
A spectrum of imaging modalities are available to assess the derangements of the knee joint. It could include X-rays, CT, USG & MRI. MRI however is the most sensitive investigation to grade the severity of the cartilage lesions. Invasive diagnostic modalities like a diagnostic arthroscopy can also be performed to know the status of the cartilage lesions.
Based on the prospective observational studies that was conducted in the department of orthopedics, patients who presented to the outpatient department or referred from elsewhere with complaints of bilateral knee pain and difficulty in walking affecting activities of their daily living were assessed. The people who were diagnosed to have either a stage 3 or 4 osteoarthritis knee. All surgically fit patients meeting the inclusion and exclusion criteria underwent either a bilateral single sitting or a staged bilateral total knee replacement based on their general health conditions. After obtaining the waiver of consent, information was gathered using a structured study proforma.
The female population was significantly more affected compared to the male population at 85.5 % vs 14.5 % respectively. This may be contributed by increased hormonal changes in older women and increased incidence of obesity. Around 52 % of our patients belonged to the age group of 61-70 years, with 23 % under 60 years and 25 % above 70 years. So that would mean that the majority of people in our study would be in the age group of 61-70 years. None of the patients included in the study had any other joint involvement.
In our study the patients had gone through conservative management which included both anti-inflammatory drugs as well as observed physiotherapy. The patients who underwent total knee replacement were the ones with no improvement in pain and function even after conservative management.
Conclusion
The minimum and maximum age in our study were 49 and 79 respectively. The gender factor when considered, it was found that females were significantly more affected compared to males. All the 48 cases under the study had pain and difficulty in performing day to day activities and x-ray findings suggestive of either a stage 3 or stage 4 osteoarthritis of bilateral knees. The OKS, The Knee Society Score and the WOMAC score showed significant improvement in the post-operative follow-up and the results were comparable between the 2 groups of patients. The mobilization was slower in the initial weeks in bilateral single sitting group. Although the single sitting bilateral Total Knee replacement patients showed a faster recovery and better functional results at 6 weeks, the functional results at 3 months and 6 months were similar. The radiological parameters also significantly improved in the post-operative assessment and no significant difference were found between the single sitting group and the staged group. The second knee of patients who underwent Single sitting bilateral TKR showed slight radiological deviations from the mean, but it was not statistically significant.
To conclude, Total knee replacement can be done as a single sitting or a staged procedure with no difference in functional and radiological outcome at 3 months and 6 months follow-up.
References
1.Primorac D, Molnar V, Rod E, Jeleč Ž, Čukelj F, Matišić V, Vrdoljak T, Hudetz D, Hajsok H, Borić I. Knee Osteoarthritis: A Review of Pathogenesis and State-Of-The-Art Non-Operative Therapeutic Considerations. Genes (Basel). 2020 Jul 26;11(8):854. doi: 10.3390/genes11080854. PMID: 32722615; PMCID: PMC7464436.
2. Dobson GP, Letson HL, Grant A, McEwen P, Hazratwala K, Wilkinson M, Morris JL. Defining the osteoarthritis patient: back to the future. Osteoarthritis Cartilage. 2018 Aug;26(8):1003-1007. doi: 10.1016/j.joca.2018.04.018. Epub 2018 May 25. PMID: 29775734.
3. Schiraldi M, Bonzanini G, Chirillo D, de Tullio V. Mechanical and kinematic alignment in total knee arthroplasty. Ann Transl Med. 2016 Apr;4(7):130. doi: 10.21037/atm.2016.03.31. PMID: 27162780; PMCID: PMC4842389.
4. Gao J, Xing D, Dong S, Lin J. The primary total knee arthroplasty: a global analysis. Journal of Orthopaedic Surgery and Research. 2020 May 26;15(1).
5. Gemayel AC, Varacallo MA. Total Knee Replacement Techniques. [Updated 2023 Aug 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538208/
6. Leitch KK, Dalgorf D, Borkhoff CM, Kreder HJ. Bilateral total knee arthroplasty--staged or simultaneous? Ontario's orthopedic surgeons reply. Can J Surg. 2005 Aug;48(4):273-6. PMID: 16149360; PMCID: PMC3211521.
7. Sikorski JM. Alignment in total knee replacement. J Bone Joint Surg Br. 2008 Sep;90(9):1121-7. doi: 10.1302/0301-620X.90B9.20793. PMID: 18757949
8. Juosponis R, Tarasevicius S, Smailys A, Kalesinskas RJ. Functional and radiological outcome after total knee replacement performed with mini-midvastus or conventional arthrotomy: controlled randomised trial. Int Orthop. 2009 Oct;33(5):1233-7. doi: 10.1007/s00264-008-0630-z. Epub 2008 Jul 25. PMID: 18654774; PMCID: PMC2899115
9. Alghadir, A.H., Iqbal, Z.A., Anwer, S. et al. Comparison of simultaneous bilateral versus unilateral total knee replacement on pain levels and functional recovery. BMC Musculoskelet Disord 21, 246 (2020).
10. Sarzaeem MM, Amoozadeh Omrani F, Omidian MM, Sahebalzamani MA, Maniei E. Clinical Outcome Comparison between Staged -Bilateral Versus Simultaneous Bilateral Total Knee Replacements. Arch Bone Jt Surg. 2021 Nov;9(6):641-646. doi: 10.22038/ABJS.2021.48053.2379. PMID: 35106328; PMCID: PMC8765198.
11. Huang YH, Lin C, Yang JH, Lin LC, Mou CY, Chiang KT, Lee MG, Chang HF, Chang HL, Su W, Yeh SJ, Chang H, Wang CC, Su SL. No difference in the functional improvements between unilateral and bilateral total knee replacements. BMC Musculoskelet Disord. 2018 Mar 21;19(1):87. doi: 10.1186/s12891-018-2006-x. PMID: 29562893; PMCID: PMC5861654.
12.Vaish A, Belbase RJ, Vaishya R. Is blood transfusion really required in simultaneous bilateral Total Knee Replacement: A retrospective observational study. J Clin Orthop Trauma. 2020 Mar;11(Suppl 2):S214-S218. doi: 10.1016/j.jcot.2020.01.014. Epub 2020 Jan 29. PMID: 32189943; PMCID: PMC7068005.
13. Lin AC, Chao E, Yang CM, Wen HC, Ma HL, Lu TC. Costs of staged versus simultaneous bilateral total knee arthroplasty: a population-based study of the Taiwanese National Health Insurance Database. J Orthop Surg Res. 2014 Jul 15;9:59. doi: 10.1186/s13018-014-0059-6. PMID: 25023777; PMCID: PMC4223718.